52 - 55












- Super User
- Category: Information
- 160
Appendix A: Full Search Strategy
Meijering, et al Appendix A - Download here.
- Super User
- Category: Information
- 247
Supplementary Appendix 1: Questionnaire for Data Collection in the Study
Supplementary Appendix 2:
- Super User
- Category: Information
- 3915
Smart et al., Appendix 1.
Note: if citing this appendix please use the citation to the original paper
Smart D, Wilmshurst P, Banham N, Turner M, Mitchell SJ. Joint position statement on atrial shunts (persistent (patent) foramen ovale and atrial septal defects) and diving: 2025 update. South Pacific Underwater Medicine Society and the United Kingdom Diving Medical Committee. Diving Hyperb Med. 2025 31 March;55(1):51−55. doi: 10.28920/dhm55.1.51-55. PMID: 40090026.
Bubble contrast echocardiography for divers. Notes regarding quality assurance
Bubble contrast echocardiography relies on the fact that microbubbles reflect ultrasound (i.e., are echogenic) and a right-to-left shunt is revealed by bubbles, appearing as white dots on the echocardiogram screen, in the left heart.
It can be a challenge to perform bubble contrast echocardiography to a high standard, because it requires that a number of actions in quick succession are performed adequately. As with all investigations, quality control is very important to ensure the lowest possible rate of false results.
Some right-to-left shunts are present without provocative manoeuvres.
To achieve a high sensitivity and greater specificity to detect a persistent (patent) foramen ovale (PFO) may require provocative testing to “open” the PFO flap at the same time as bubble contrast is present in the right atrium. This requires a co-operative patient, co-ordination between operator and patient, and precise timing.
PROCEDURE
After obtaining informed consent, that should be suitably documented, insert a venous cannula of at least 20-gauge size. A vein in an antecubital fossa should be used, so that blood can be drawn back into the syringe and so that rapid injection has a short transit time to the heart.
The arm in which the cannula is placed should be elevated to above the height of the heart, so that gravity facilitates rapid passage of the bubble contrast into the right atrium, which ensures better opacification of the chamber with the contrast. The patient is usually in the left lateral position to obtain apical four-chamber images using transthoracic echocardiography. If the cannula is in a right antecubital vein and the arm is rested along the right side of the patient, the cannula will be above the height of the heart. If a left antecubital vein is used, the left arm should be supported above the height of the right atrium.
Injection of bubble contrast into a left arm vein has the advantage that it will detect a right-to-left shunt associated with a left superior vena cava draining to the left atrium, if one is present.
Bubble contrast should be formed by using a three-way tap, attached to the back of the cannula (and not the injection port), with two Luer lock 10 mL syringes. One syringe should contain 7-8 mL of normal saline, 1 mL of air, and 1 to 2 mL of blood withdrawn through the cannula into the syringe. The resulting 10 mL should be forcibly pushed back and forth from one syringe to the other 10-15 times until macroscopic gas is replaced by microbubbles (Figure 1). Before injection, the saline, blood and bubble “contrast” should be moved to one of the syringes, and the syringe should be held with the plunger up, so the last mL containing excess air is not injected. The presence of blood in the contrast seems to stabilise the bubbles, so that they persist as microbubbles for longer in the circulation.
Figure 1
Demonstration of creation of microbubbles in a mix of the patient’s blood and sterile saline

In Figure 1, the intravenous cannula is placed in the left antecubital fossa and secured. The 3-way tap is attached to Luer-lock syringes and the contrast is made by forcing the blood, saline and air mixture between the two syringes. On injection the syringe is held upright so any excess air is not injected.
The initial injection of bubble contrast should be given during normal breathing. The contrast should fill the right atrium and right ventricle, such that the white appearance of the bubbles provides complete opacification, with no “black” (non-echogenic) blood visible between the white bubbles (Figure 2). If there is a large atrial right-to-left shunt and there is complete opacification of the right atrium with bubble contrast, microbubbles may be seen crossing the atrial septum during each normal inspiration. If so, a single injection of bubble contrast may be adequate to confirm that there is an atrial shunt (Figure 2).
Figure 2
(panels A-F). Apical four chamber images during bubble contrast echocardiography when a patient with a PFO breathed normally. Bubble contrast is bright white and blood is black
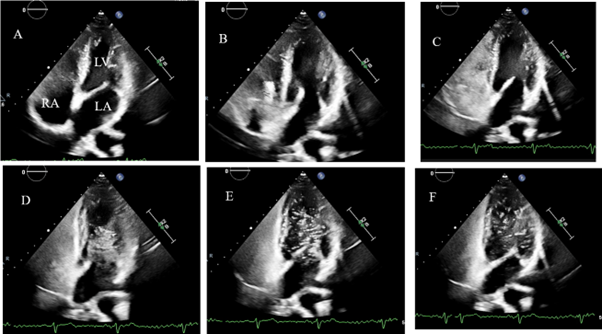
In Figure 2, the contrast can be seen entering the right atrium (RA) in panel B and C. By panel D, there is already a bolus of contrast in the left ventricle (LV) spontaneously, indicating a resting right-to-left shunt. The white contrast is densely opacifying the right heart, and is filling the RA along the whole atrial septum. The left atrium (LA) is not very opacified as the bubbles are entering the LV as soon as they cross the septum.
Sometimes an area of bubble-free black is seen adjacent to the atrial septum. This is due to the inflow of blood that does not contain microbubbles from the inferior vena cava: for many patients the Eustachian valve or Chiari network direct the inferior vena cava blood towards the atrial septum, as occurs in foetal life. If there is right-to-left shunting across a PFO, it will not be detected if the blood in the right atrium that is adjacent to the atrial septum is free of bubble contrast. In order to ensure that bubble contrast is adjacent to the atrial septum, provocative manoeuvres may be necessary, and in addition altering the position of the patient by either lying them flatter, or propping them up more, can result in more complete filling of the right atrium with bubble contrast.
PROVOCATION MANOEUVRES AND QUALITY CONTROLS
Even if the initial resting injection shows a right-to-left shunt, further injections are usually necessary to confirm that the shunt size increases with provocative manoeuvres. A bubble contrast injection with a sharp sniff as soon as the right atrium is completely filled with contrast will often open a PFO to reveal a right-to-left shunt, which was not seen during normal breathing, or to increase the amount of shunting. A sniff reduces the intrathoracic pressure suddenly, and the shunt is seen immediately after the sniff. A large number of bubbles entering the left heart following a sniff is diagnostic of an atrial shunt (a PFO or atrial septal defect), rather than a pulmonary shunt. Furthermore, the presence of a shunt with only a sniff indicates that only a small amount of pressure change is required to open a PFO and cause a right-to-left shunt.
Release of a Valsalva manoeuvre is also used to provoke right-to-left atrial shunting (Figure 3). It is important to ensure that there is opacification of the right heart with bubble contrast immediately after the Valsalva release. To ensure that happens the bubble contrast should be injected immediately before the patient starts the Valsalva manoeuvre. To obtain accurate results requires careful performance of the Valsalva release.
Figure 3
(panels A-F). Bubble contrast echocardiography in the same patient as in Figure 2, showing an increase in the shunt with a Valsalva manoeuvre
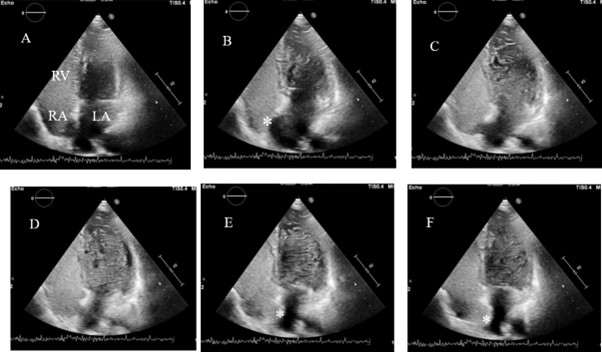
Figure 3 shows the same patient during a Valsalva manoeuvre, echo images A-F. The right ventricle (RV) and RA are densely opacified with contrast and in panel B, the atrial septum (*) is bulging towards the RA because at that time the LA pressure is higher than RA pressure at rest. In panels E and F, after release of the Valsalva manoeuvre, the septum (*) is seen to bulge towards the LA, because the LA pressure is lower than the RA pressure. The degree of excursion of the septum indicates the presence of an atrial septal aneurysm or floppy septum that is associated with a larger PFO. In this case the shunt is very large because there is almost completely opacification of the LV with the white bubbles.
The patient is instructed to perform a Valsalva by stopping breathing in a neutral position (so the echocardiographic image is not obscured by the presence of fully inflated lung tissue in the path of the ultrasound beam from the transducer to the patient’s heart), to hold their nose tightly and to close their mouth tightly. The patient is then asked to strain by trying to forcefully exhale, whilst maintaining complete closure of the nose and mouth. It can be helpful to tell the patient to imagine that there is a pressure gauge in the middle of the chest and the pressure should be elevated and maintained at a high level for a period of time, until they are told to release the strain. The patient should maintain the strain until the cardiac chambers appear visibly smaller on the echocardiogram monitor because of the reduction in venous return.
When the cardiac chambers are seen to be smaller the patient is asked to release the Valsalva suddenly, and go back to breathing normally without making large inspiratory or expiratory breaths. At the moment of Valsalva release, one expects to see microbubbles stream rapidly into the right heart, causing complete wall-to-wall opacification of the right heart, and to see the atrial septum bulge across towards the left. At that moment the right atrial pressure has recovered, but the left atrial pressure should still be low. If there is a PFO, a bolus of bubbles would be observed crossing the atrial septum into the left heart at that time, or in one of the next couple of cardiac cycles. If no right-to-left shunt is seen after the first bubble contrast injection with Valsalva release, the procedure should be repeated at least twice more, and possibly up to five times in total, before the test is reported as negative.
Changes during a Valsalva manoeuvre are as follows. At the onset of Valsalva (straining against a closed airway), the intrathoracic pressure is increased and exceeds venous pressure. That causes reduction of venous return to the right atrium. During about 10 seconds, both left and right ventricles can be seen to reduce in size and there is a reduction in the number of bubbles appearing in the right heart. Thus, to quality control the Valsalva manoeuvre, it is important to see reduction in size of both left and right heart chambers, and to see that the flow of bubbles back to the heart decreases.
When the Valsalva is released suddenly, the intrathoracic pressure decreases immediately. This leads to rapid reduction of the pressures in both atria. The right atrium is able to fill rapidly from the venous circulation, which at that time is opacified by bubble contrast. However, the left atrial pressure remains low, because the pressure in the pulmonary veins is also low. Because the right atrial pressure and filling recover more quickly than the left atrial pressure and filling, one often sees the atrial septum bowing towards the left atrium (Figure 4).
Figure 4
(panels A and B). Larger format image to demonstrate excursion of the atrial septum (*)
In Figure 4 panel A, there is dense and complete opacification of the right heart with contrast with no gaps between bubbles and with the bubbles being right up against the atrial septum (marked as *). In panel B, the atrial septum (*) is bulging towards the left heart and bubble contrast is easily seen in the LV. This shows the quality of bubble contrast and provocative testing that is required, and how a substantial (some call a Grade 4) shunt appears. There is no need to attempt to count the bubbles in the left heart in shunts of this magnitude.
The quality control when the Valsalva manoeuvre is released requires seeing that the right atrium has dramatically filled with dense bubble contrast, but the left heart remains small. If bubble contrast is not present in the right atrium adjacent to the atrial septum, and the septum does not move to the left, the investigation may be inadequate.
Because the haemodynamic changes necessary to open a PFO may vary from patient to patient, it is recommended to make alterations to the duration of the Valsalva manoeuvre, and also consider moving the patient's position, if there is lack of opacification of the right atrium at the time of Valsalva release.
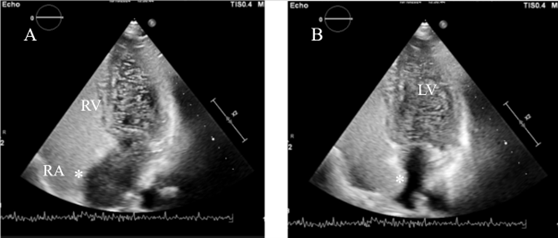
Figure 5
(panels A-F). Apical echocardiogram images before and during a Valsalva manoeuvre
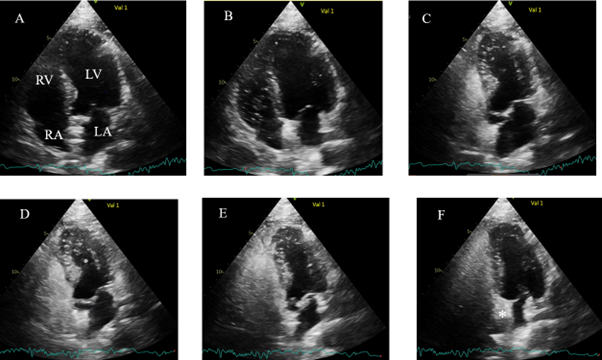
Figures 5 and 6 show an apical echocardiogram view during a Valsalva manoeuvre and immediately after release. In panels A and B, the LV is of normal size. Contrast appears in the RA and RV in panel C. In panels D and E, during the Valsalva manoeuvre, the LV and LA are much smaller because of the reduction in venous return, so the inflow to the heart is reduced. In Panel F the atrial septum (*) is bulging towards the LA because immediately after the release of the Valsalva manoeuvre the RA fills before the LA. An occluder device can be seen in the atrial septum, as this study was performed 6 months following PFO closure.
Figure 6
(panels G-J). Apical echocardiogram images with left ventricle returning to normal size after release of the Valsalva manoeuvre
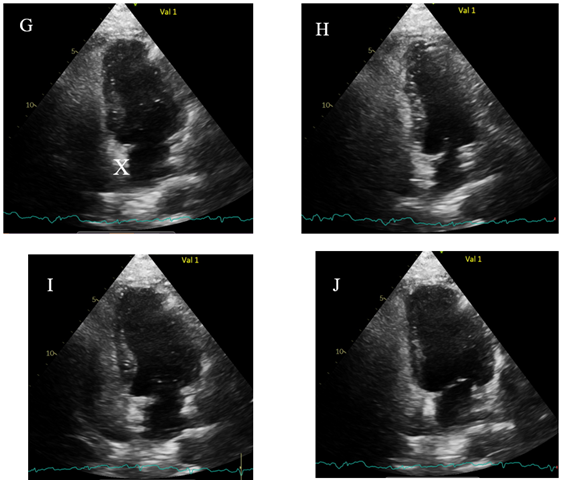
A Gore Cardioform Septal Occluder device (X) can be seen in the atrial septum in panel G, with the device also bulging towards the LA, proving that the RA pressure is greater than the LA. In panels G - J, the LV returns to a normal size. Only occasional bubbles are seen the in the LV representing a tiny residual shunt of no concern. To be certain the Valsalva is effective in reducing venous return, it is important to see the LV reduce in size and to confirm by seeing the bulging of the septum towards the LA.
POTENTIAL FALSE NEGATIVE AND FALSE POSITIVE TESTS
It is essential for quality control that the echocardiogram window provides good images of the heart at the time when one expects bubbles to cross into the left heart. The left heart should be visible and recordable at the time of the sniff and for a few cardiac cycles afterwards. It can be difficult to keep the images of the heart in the image window during Valsalva release when the patient’s intrathoracic pressure changes and the heart changes its position relative to the chest wall (where the ultrasound probe is held), and the patient is likely to move a little. If the echocardiogram image cannot be maintained at the time when a shunt is expected, it can lead to false negative results.
Caution should be exercised when interpreting the appearance of bubbles in the left heart after the provocative manoeuvres, because they may result in a false positive diagnosis of an atrial shunt. When bubbles appear more than 3 cardiac cycles after Valsalva release or a sniff, or if a shunt is present during respiration at rest, the shunt may be trans-pulmonary; either traversing a large arteriovenous malformation or multiple microscopic vascular shunts. If the late shunt appears after Valsalva release, when multiple injections have already been given (and the pulmonary capillaries have trapped many bubbles), a few bubbles can sometimes be seen in the left heart in a patient with normal heart and lungs; this is likely to be a false positive test.
False positive tests can also occur if colloid based contrasts are used. Gelofusine® forms smaller bubbles that will pass through a normal pulmonary circulation.
Figure 7
(panels A and B). Apical echocardiogram images showing occlusion of the PFO
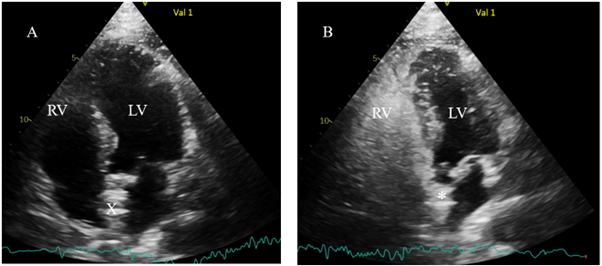
In Figure 7, panel A has no contrast and shows a normal size LV, and the closure device (X) in the atrial septum centrally placed between RA and LA Panel B shows that immediately after Valsalva release, the LV is smaller and the atrial septum (*) is bowing towards the smaller LA. The right heart is full of dense contrast, but the LV has no contrast, showing good occlusion of the PFO.
TO SUMMARISE THE QUALITY CONTROL:
1. An apical view of the heart should be maintained throughout the bubble contrast injection and provocative manoeuvres.
2. In order to ensure rapid arrival of bubbles at the right atrium, bubble contrast should be injected into a vein in an antecubital fossa, with the vein positioned above the level of the right atrium.
3. Bubble contrast should be formed by mixing saline with a small amount of the patient’s blood and a small amount of air.
4. Bubble contrast should completely opacify the right side of the heart so that it appears white. No “black” (non-echogenic) blood should be visible between the bubbles in the right heart.
5. The bubble contrast should be adjacent to the atrial septum at the time of provocative manoeuvres.
6. Valsalva manoeuvres should be quality controlled to ensure that all cardiac chambers reduce in size during the pressurisation of the chest; and on release, the bubble contrast should rush into the right side of the heart and fully opacify the right atrium adjacent to the septum, and the atrial septum should be seen to bulge towards the left atrium, confirming that the right atrial pressure exceeds the left atrial pressure.
- Super User
- Category: Information
- 257
Stevens, et al. Appendix 1
Diver telephone triage health questionnaire.
Telephone/ Contact Triage Sheet -Project ID 24772
Subject Number:
1. Are you aged 18 years or over?
2. What was the date of your last dive?
3. Do you currently suffer from any health issues?
4. Are you currently able to exercise at your maximum capacity?
5. Have you ever had or do you now have any health issues or injuries that stopped you diving?
6. Have you had any breathing difficulties in the last 12 months?
7. Do you currently have lung disease, chest infections, asthma, emphysema or excessive shortness of breath when exercising?
8. Have you ever had or do you now experience heart problems, chest pain or palpitations?
9. Do you currently have a respiratory or throat infection, ear clearing problems or sinus pain?
10. Are you currently taking any prescription or over the counter medications? Please define if so
11. Do you suffer from migraines or headaches?
12. Have you experienced any seizures or episodes of loss of consciousness?
13. Are you currently pregnant?
14. Have you experienced any injury, trauma or surgical procedures in the last 12 months?
15. Have you experienced any other health issues not mentioned above?
16. Are you currently completely well?
17. Do you dive 20 or more times per year?
Proceed Y or N ? Study Doctor Sign_____________________Date_______________
- Super User
- Category: Information
- 328
Appendix 1. Detailed descriptions of diver histories.
All audiograms for the cases are summarised in Appendix 2. The original copies of the audiograms have been withheld for privacy and anonymity.
Case 1
A 51 YO male scientific diver (Body Mass Index (BMI) = 26 kg/m2) with a normal audiogram at last medical. He was competing in an underwater hockey tournament and presented with hearing loss and tinnitus in the right ear (maximum depth 2.4 m). There were no vestibular symptoms. The subject had no previous issues or injuries to his ears from underwater hockey or diving, and all audiograms for his previous 20 years’ scientific diving medicals were normal. No compressed air diving had been undertaken in the week before or during the tournament. He was completely well before the tournament and denied any respiratory symptoms. Following the first day’s competition, he noted painless reduced hearing and tinnitus in his right ear. There were no ear clearing problems or other impact/injury. He played a further 6 games over 6 days with no change in his symptoms. After consulting a diving medicine specialist, an AC/BC audiogram was performed day 7 by an independent audiologist, before assessment day 8. Both tympanic membranes were normal appearance and the subject could demonstrate normal ear clearing. There were so symptoms or signs of vestibular disturbance, and full neurological examination was normal. The left ear was unaffected. The right ear audiogram was consistent with a mild to severe down-sloping sensorineural hearing loss affecting 1-8 kHz. No imaging was undertaken.
The diver’s case information was discussed with an Ear Nose and Throat (ENT) specialist, but was not reviewed in person by that specialist. In view of the likely causation from breath hold diving to 2.4m, a diagnosis of inner ear barotrauma was made. He agreed to a trial of HBOT following detailed instruction to undertake very gentle ear clearing. The subject was provided 9 treatments of HBOT, at 2.43 kPa (14:90:20 table, 3 x 5-minute air breaks). Prednisolone 50 mg daily was commenced day 2 after the second HBOT. No other specific treatment was advised apart from avoiding strong Valsalva manoeuvres and heavy lifting. Following two HBO treatments within 24 hours, and a single oral prednisolone dose, the subject’s hearing returned to normal range for 1kHz to 2kHz and had significantly improved in 3 and 4 kHz. He received ENT assessment with no changes to management. HBOT was continued daily to a total of 9 treatments. At no stage did he develop any vestibular symptoms. By end of 9 treatments, hearing in the right ear was normal for all frequencies except 6 kHz and 8 kHz. The subject received follow-up at 3, 6 and 12 months and his hearing has remained stable. After assessment by ENT and Diving Medicine Specialists, he was cleared for returning to occupational diving. He successfully resumed all diving activities including underwater hockey and has had no further issues with hearing.
Case 2
A 22 year-old male commercial diver (BMI = 24 kg/m2) had an uneventful 4-year diving career with more than 300 hours spent underwater. He received a comprehensive AS/NZS 2299.1 occupational diving medical one day prior to his incident, and did not dive that day. At that assessment, he demonstrated normal ear clearing, tympanometry and his audiogram was normal. He had no respiratory symptoms at the time of the medical and none on the day following. He undertook two brief dives the day after his medical, to 18 metres for 5 minutes each. The dives were separated by a surface interval under 15 minutes (a common practice for the industry). The diver noted no ear clearing difficulties, ascents were fully controlled and no symptoms were noted during or after the dive. He did not experience vertigo or disequilibrium at any stage, before, during or after the dives, and no lifting, straining, forced Valsalva, coughing or sneezing occurred. He was well when retiring to bed the same night. The next morning, he woke with hearing loss and tinnitus in his left ear. Of his own volition he returned to the same audiologist who had performed his AS/NZS 2299.1 audiogram, and asked for a repeat test. This demonstrated 60-85dB sensorineural hearing loss across all frequencies from 500 to 8 KHz. An urgent ENT/diving medicine assessment revealed normal tympanic membranes normal middle ear function and a negative fistula test, completely normal neurological examination, no nystagmus and sharpened Romberg test stable for 60 seconds. He agreed to a trial of HBOT following detailed instruction to undertake very gentle ear clearing. No imaging was undertaken before treatment. He was provided with a 14/90/10 hyperbaric oxygen treatment table the night of his presentation. Improvements in hearing were noted of 15-30dB across frequencies 500Hz-3KHz, immediately after the first treatment. It was decided to continue HBOT on a daily basis and Prednisolone 50mg was prescribed after the second HBO treatment. By day 10 (10th HBOT), hearing had improved in the left ear, with mild impairment only in 6-8kHz. High resolution CT scan of his petrous temporal bones was normal. He was reviewed by an ENT specialist, and no further treatment was advised. His hearing recovery persisted to 8 months at follow-up. After detailed discussion regarding his diving career, it was decided to advise against further diving. He is reconfiguring his career to train as a Ship’s Master.
Case 3
A 52-year-old recreational snorkeler (BMI not calculated, but not clinically obese) had a previous history of high frequency hearing loss from 3 – 8 kHz due to industrial noise. He was breath-hold diving for abalone and crayfish to a maximum of 4-5 metres depth. He undertook multiple descents and ascents over a 30-minute period. He experienced difficulty in clearing both ears and experienced pain and diminution of hearing in his right ear. He had no vertiginous symptoms. He denied respiratory symptoms prior to his breath-hold dives. He presented to his GP who referred him to an ENT specialist. After a normal MRI scan, he was prescribed 50mg prednisolone daily for 10 days. After no benefit from steroids, he was then referred for HBOT. His audiogram at the commencement of HBOT was identical to post injury 10 days before, demonstrating 55-70 dB sensorineural hearing loss across all frequencies right ear. Neurological examination was normal, with no signs of vestibular dysfunction. Middle ear clearing was normal at the time of diving specialist assessment. Given failure to improve with steroids, HBOT was commenced as a possible salvage. He was provided 10 daily HBOT using 14/90/20 or 14/90/10 schedules. There was normalisation of his hearing in 500-1.5 kHz and significant improvement of 2 kHz, following three hyperbaric oxygen treatments. He completed the 10 treatments and at discharge, was counselled against further breath-hold diving. His hearing remained stable at follow-up 6 months after treatment.
Case 4
A 31-year-old male commercial diver (BMI = 27 kg/m2) with 10 years’ experience, had a previous history of mild musculoskeletal decompression sickness, seven years prior to presentation. His previous annual dive medical health risk assessment showed normal hearing nine months before his injury. He had no symptoms or ear issues in the ensuing months. Just before his presentation, he been diving daily within dive table limits over a four-day period. There was no strenuous activity, no trauma, no ear clearing problems during his diving, and no respiratory symptoms. On the fourth day, starting with repetitive factor 1.0, he completed a single dive (with five-minute safety stop) to 15m for 53 minutes – he had no ear clearing issues and was symptom free immediately post dive. The evening after his dive, he noted reduced hearing in his right ear, “like water in the ear”, but did not report his symptoms until three days later (this period spanned a weekend). After reporting, his supervisors referred him for medical assessment. He had no symptoms or signs of vestibular dysfunction, no nystagmus, normal balance, normal tympanic membranes which cleared easily with gentle Valsalva, negative fistula test. His audiometry at day four showed sensorineural hearing loss in his right ear at four days post-diving across 500 Hz – 8 kHz. Impedance audiometry showed normal middle ear pressure with increased tympanic compliance. Findings were consistent with sensorineural hearing loss right ear, probably due to IEBT, however isolated cochlear decompression illness (although unlikely) could not be absolutely ruled out. Following discussion with ENT specialists, he was treated with a series of 14/90/20 tables for 10 consecutive days. Steroids were not prescribed. Audiometry was independently undertaken at the hospital’s audiology service, returned to normal after HBO treatment four. His hearing has remained stable and normal to 3 months follow up.
He received an MRI scan of his brain which demonstrated no abnormalities in his cranial nerves 7 and 8, and membranous labyrinth, and an incidental tiny cyst in the right sella turcica. High resolution CT scan was normal except for a slightly narrow right cochlear aqueduct (of uncertain significance). Following review and discussions with his employer, he chose not to dive again.
Case 5
A 62-year-old male hyperbaric professional (BMI = 27), with 3,500 hours recreational diving experience and no previous ear issues or barotrauma. Previous audiograms for occupational medicals had been normal with all frequencies demonstrating 20 dB or less hearing loss. Two uneventful dives were completed day one, well inside no-decompression limits, to maximum 21 m depth. The diver noted mild upper respiratory symptoms at the start of day 2. Following a 21-hour surface interval (at 0926), an uneventful multilevel dive was undertaken day two to 16 metres for 64 minutes, average 11.3 metres including five minutes at 3-5 metres safety stop. The diver had no problems clearing his ears on the first dive, day two. After a one-hour surface interval a second dive was commenced to 16 metres. The diver made camera adjustments whilst descending and omitted ear clearing. He noted pain in his right ear, which settled after some sub-surface ascents and further descent. The dive was completed with no further issues and no reverse ear squeeze, 57 minutes dive including a five-minute safety stop at 3-5 m. During the afternoon, the diver snorkelled with a number of free dive descents, and noted right ear stickiness when clearing. He noted a minor hearing impairment and crackling that evening. The diver woke the next day with significant hearing impairment and tinnitus in the right ear, and 2/10 pain. He was unable to hear conversation with the right ear when his left ear was occluded. He did not dive or snorkel again and flew home to Australia day 10 without ear clearing difficulties, although with some perception of moist crackling in the middle ear. Following air and bone conduction audiograms, he was assessed by an ENT specialist who diagnosed inner ear barotrauma with moderate sensorineural hearing loss. At the diver’s request, he was referred for HBO treatment, and received 5 daily treatments using 14:90:10 tables, and had no difficulties in clearing his ears. The diver chose to stop HBOT at treatment number 5, because hearing in the right ear had returned during treatment 2. Steroids were not prescribed. No imaging or further investigations were performed. He returned to diving one month later and has completed 65 more dives in 2023-24 without incident.