52 - 55












- Super User
- Category: Information
- 415
Appendix 1 – CRAO Questionnaire
1. Does your HBU accept and treat patients presenting with CRAO?
2. How many CRAO cases have you treated in the last 5 years?
3. Is there is time window from onset of symptoms beyond which your facility will not offer HBOT?
4. What are the diagnostic criteria/minimum requirements by your facility before commencing HBOT?
5. What initial treatment table do you offer for CRAO? 18:60:30 or similar, TT5, 140 :90, other (please list)
6. What follow-up HBOT schedule and tables do you use?
7. Is the patient admitted into hospital if a diagnosis of CRAO is made and the patient has HBOT?
8. Are they on high flow oxygen initially?
9. Are they on high flow oxygen between treatments?
10. Would the hyperbaric treatment schedule vary between physicians at the department or is there a unit consensus on treatment schedule?
11. Does hyperbaric treatment vary according to patient’s symptoms?
12. Is there a specific number of hyperbaric treatments that get offered, or does it vary according to patient response?
13. If there is a variation, please can you outline this treatment plan?
- Super User
- Category: Information
- 623
Appendix 1. Aide memoire for diving deaths in Tasmania
Deceased
|
Important requirements |
Notes | |
|
The body to remain in clothing or dive suit. The body will be transported directly to the Royal Hobart Hospital (RHH) (preferred) or nearest hospital, weather conditions permitting. |
The body may need to be extracted by land or air transport and may need to be taken to another hospital on route for testing to occur, depending on duration since the death. Other venues for initial assessment include: Launceston General Hospital (LGH), North West Regional Hospital (NWRH), Mersey Community Hospital (MCH), West Coast District Hospital (WCDH), King Island District Hospital (KIDH), and Flinders Island Multipurpose Centre (FIMC). |
The Coroner’s Associate is to ensure appropriate transportation of the body in keeping with time critical body analysis requirements. |
|
If Forensic Services do not attend the location, they will attend the Mortuary for photographs after the CT etc. has been done. |
This step is dependent on ad-vice from the Forensic Pathologist/Coroner as to the value of Mortuary photographs to their exam/investigation. | |
|
The body is to be transported to an appropriate hospital for CT scan or erect CXR within three hours at best (maximum of eight hours) of death. |
If body is unable to be trans-ported in this time, the Coroners Associate will liaise with the RHH Hyperbaric Consultant/Registrar as to any alternatives. |
The RHH hyperbaric Consultant/Registrar will make the arrangements at the alternative venue. The Coroner's Associate will organise the transport. |
|
The Mortuary Ambulance or other transport will deliver the body to the RHH or other venue within considered time constraints. |
The RHH Hyperbaric Consult-ant/Registrar will provide advanced notice of the body arriving for CT scanning/CXR to the respective hospital through the Executive Director of Medical Services (EDMS) or Tasmanian Coordinator for Ochre Medical Services, Queenstown/KI/FI. |
Once these tests have been completed, the Police Officer will accompany the body to the Mortuary for admission. The usual process of body delivery to the RHH will then occur, should the body require an urgent CT scan outside RHH. |
Equipment
|
Important requirements |
Notes | |
|
Secure the diving equipment with video +/- photo documentation. |
Body worn camera (BWC) to be activated and to remain on during the incident. |
Specifically – mask, snorkel, wet suit, fins, weight belt/pouches, BCD, catch bag, scuba apparatus, hookah/surface supply apparatus, and dive watch/computer. (Please refer to Dive Incident Inventory form). |
|
If there is SCUBA in use – seal the equipment with the valves closed: to turn off the gas canister/cylinder count and record the number of rotations of the valve taken to seal the SCUBA tank/gas canister/cylinder. For Rebreather equipment, the two-way cock in the mouth piece needs to be turned to 'atmosphere' (to capture the gas inside the canisters and hoses) and taped in position. Tape all moveable parts in the position they were in for the dive, apart from the above (to be taped in the new position). |
The items need to be left in their current state (i.e. not to be disassembled, or if disassembled to not be reassembled) to be investigated by the Technicians of the RHH Department of Diving and Hyperbaric Medicine (DDHM) as deemed appropriate. |
Southern Marine and Rescue Services (MRS) can dry equipment or assist with wet weighing, if necessary. |
|
All diving and other equipment seized at the scene will be brought to Hobart for assessment and storage at MRS. Boats may be seized if they are relevant to the investigation e.g. Fixed SSBA/Hookah set up on a boat. |
Preference for Dive Squad Supervisor to attend and secure/seize equipment. Issue receipt for any equipment seized. Continuity labels to be attached. |
Forensic Services can have members trained to secure the equipment in the event Dive Supervisor does not attend. Forensic Services may also take the necessary equipment to MRS. |
|
If Forensic Services did not attend scene, MRS can attend on their behalf and photograph equipment. |
If there is a diver from MRS attending, then it will be left to them to secure the equipment in the best way for examination by the DDHM Technicians. Forensic Services can attend MRS prior to the equipment being sent to the RHH DDHM in order to comprehensively photo document all essential equipment. |
Further photographs and the use of drones at the scene can be completed at a later date, if needed. |
|
MRS are to coordinate the inspection of equipment by RHH DDHM Technicians. |
Specifications relating to equipment movement will be outlined in this document and if there is any confusion, advice will be sought from the Dive Squad Supervisor via the Coroners Associate. |
Once any boat assessment is completed it may be considered for conditional release under a Coronial Care and Control Order. |
Appendix 2. Diving Deaths Checklist
|
Item |
Notes |
|
Dive Cylinder / spare |
When in use, the cylinder valve should be fully open & back half turn. When diving, a loose valve is considered ‘open’, hence the term ‘fully open & back half a turn’ = ‘loose’, whereas a tight valve is considered ‘closed’. Be aware some individuals are incorrectly opening valves to the hard stop. This can give a false indication of a closed valve. This can cause a pressure lock when trying to remove the regulator, as the valve is actually open, and system pressurised. Caution is advised. Cylinder valves should be used when fully open, this prevents a narrowed orifice freezing over and allows gas to flow freely. Turn valve off clockwise & note number of full turns. Isolate spare cylinder for air analysis comparison. |
|
1st and 2nd stage regulators |
Check & record pressure gauge. Tape in found position, all adjustment knobs on 2nd stage demand valves. Check for neck strap. |
|
Buoyancy compensator |
Note method of inflation, power inflator (connected to 1st stage regulator), small cylinder or cartridge. Maintain integrity as found. Do not drain contents. Note and record presence or absence and amount of integrated weights if relevant. |
|
Face mask |
If full face mask, check connections, note vent position, note any adjustments or isolation. Do not rinse or wash out mask / oral nasal. |
|
Snorkel |
Do not wash/ rinse. |
|
Swim fins/ boots |
Collect fins, if wearing boots check for weighted soles and release devices. |
|
Dive computer |
Remove from water/ wet area to stop recording. Turn off. Dry and bag. |
|
Wetsuit/ drysuit |
Collect all wetsuit parts worn by deceased for buoyancy assessment. |
|
Weight belt |
Collect weight belt, pocket weights, or weight harness. If deceased, photo in situ. |
|
Deco tables/ docs |
If available, collect full dive plan, decompression & repetitive diving worksheets. |
|
Camera equipment |
Collect recording devices, cameras / video. Check for recordings, memory discs etc. |
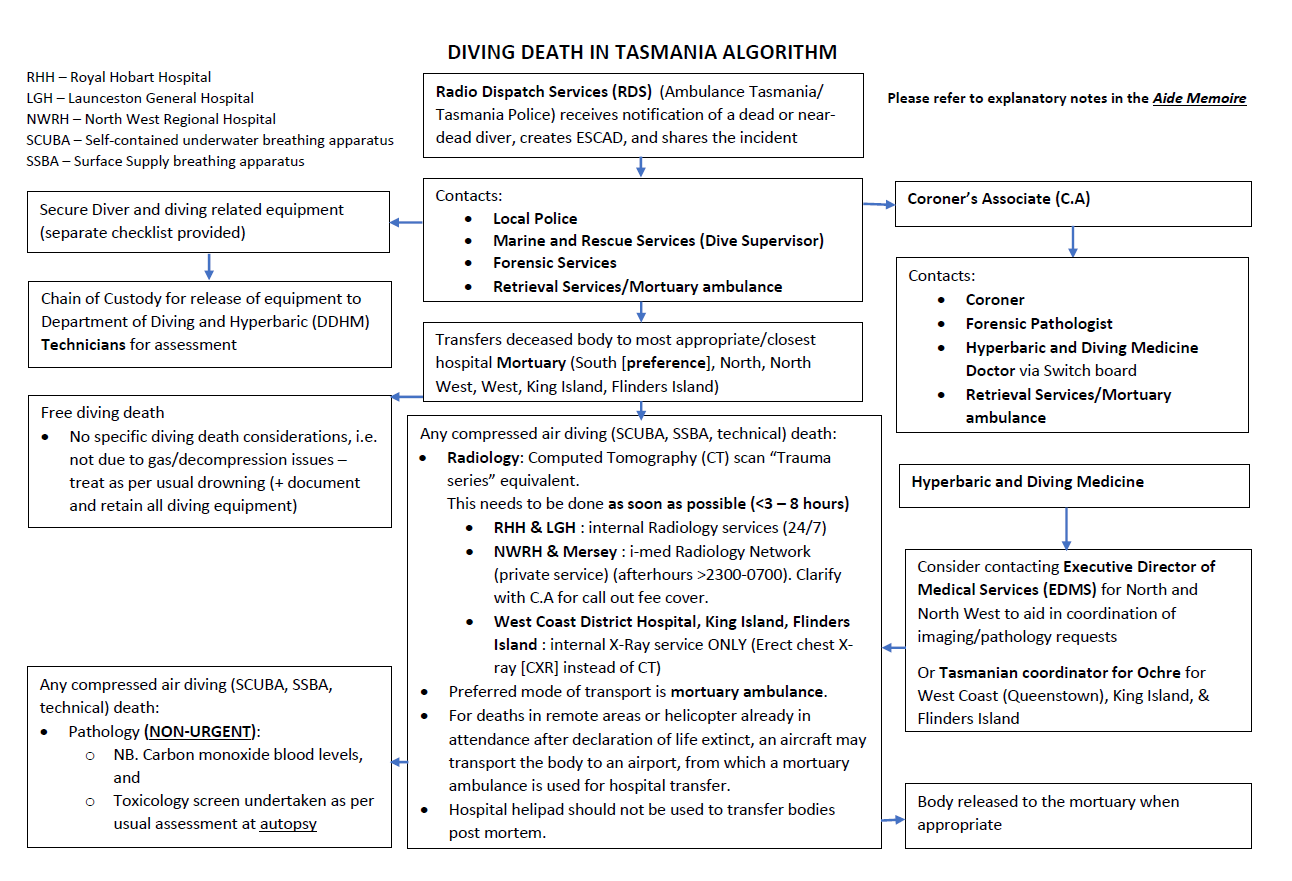
Appendix 3. Diving Death in Tasmania Algorithm
- Super User
- Category: Information
- 197
Appendix 1: Search Strategies
Database: Ovid MEDLINE(R) and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily <1946 to October 11, 2021>
Search Strategy:
1 Hyperbaric Oxygenation/ (12,257)
2 hyperbaric oxygen*.tw,kw. (10,610)
3 hyperbaric chamber.tw,kw. (774)
4 (HBO2 or HBOT).tw,kw. (2,401)
5 or/1-4 (15,864)
6 randomized controlled trial.pt. (546,028)
7 controlled clinical trial.pt. (94,451)
8 randomi?ed.ab. (641,941)
9 placebo.ab. (222,177)
10 clinical trials as topic.sh. (197,707)
11 randomly.ab. (367,604)
12 trial.ti. (249,184)
13 or/6-12 (1,440,457)
14 animals/ not humans/ (4,863,110)
15 5 and 13 (1,494)
16 15 not 14 (1,132)
Database: Embase Classic + Embase <1947 to 2021 October 11>
Search Strategy:
1 hyperbaric oxygen therapy/ (3,786)
2 hyperbaric oxygen/ or hyperbaric chamber/ (16,071)
3 hyperbaric oxygen*.tw. (11,957)
4 hyperbaric chamber.tw. (952)
5 (HBO2 or HBOT).tw. (3,235)
6 or/1-5 (20,132)
7 crossover-procedure/ or double-blind procedure/ or randomized controlled trial/ or single-blind procedure/ or (random* or factorial* or crossover* or cross over* or placebo* or (doubl* adj blind*) or (singl* adj blind*) or assign* or allocat* or volunteer*).tw. (2,565,990)
8 (animals/ or animal experiment/ or animal model/) not humans/ (3,621,497)
9 6 and 7 (2,288)
10 9 not 8 (1,749)
Database: EBM Reviews - Cochrane Central Register of Controlled Trials <July 2018>
Search Strategy:
1 Hyperbaric Oxygenation/ (390)
2 hyperbaric oxygen*.tw,kw. (1,320)
3 hyperbaric chamber.tw,kw. (120)
4 (HBO2 or HBOT).tw,kw. (370)
5 or/1-4 (1433)
CINAHL
|
|
|
- Super User
- Category: Information
- 1139
DRAFT
Wackett J, Devaney B, Chau R, Ho J, King N, Grewal J, Armstrong J, Mitra B. Reported outcome measures in necrotising soft tissue infections: a systematic review. Appendix 1 - 3.
Appendix 1: A supporting document that outlines the search strategy employed in our OVID Medline search so that the search could be repeated and readers can better understand our search terms
- Fasciitis, Necrotizing/
- Fournier Gangrene/
- Gas Gangrene/
- Necrot?ing soft tissue infection*.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms]
- Fasciitis, necrotic?ing.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms]
- Fournier gangrene.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms]
- Gas gangrene.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms]
- 1 or 2 or 3 or 4 or 5 or 6 or 7
- limit 8 to (English language and humans and last 10 years)
Appendix 2: A supporting document that provides references for the studies ultimately included by our review for data extraction
Appendix 3: A supporting document that lists all outcome measures and their relative frequency that were identified by the study, having been stratified into groups based on their content. This list provides readers with a comprehensive account of outcomes currently being reported in NSTI research should they need it for further work
- Super User
- Category: Information
- 6511
Draft
Equipoise: an important ethical consideration when contemplating participation in a randomised controlled trial of hyperbaric oxygen treatment in necrotising soft tissue infections
Bridget Devaney1
1 Department of Intensive Care and Hyperbaric Medicine, Alfred Health, Melbourne, Australia
Corresponding author: Dr Bridget Devaney, Head of Hyperbaric Medicine, Alfred Health, 55 Commercial Road, Melbourne, VIC 3004, Australia
ORCID ID: 0000-0001-6521-418X
Keywords
Clinical Trials; Ethics; Hyperbaric research
Abstract
(Devaney B. Equipoise: an important ethical consideration when contemplating participation in a randomised controlled trial of hyperbaric oxygen treatment in necrotising soft tissue infections. Diving and Hyperbaric Medicine. 2024 31 March;54(1):NN−nn. doi: 10.28920/dhm54.1.NN-nn. PMID:????)
A proposal for a large, multi-centre, randomised controlled trial investigating the role of hyperbaric oxygen treatment (HBOT) in necrotising soft tissue infections (NSTI) has led to much discussion locally and internationally about whether participation is ethical for a centre where stakeholders already consider HBOT standard practice. This article systematically addresses the concept of clinical equipoise specific to the role of HBOT in NSTI, and presents a series of considerations to be taken into account by key stakeholders at potential participating sites.
Introduction
Highly regarded and widely published Danish colleagues are in the advanced phases of planning a multinational randomised controlled trial (RCT) investigating the use of hyperbaric oxygen treatment (HBOT) for necrotising soft tissue infections (NSTI). The trial involves patients with NSTI being randomised to receive either standard care (surgical debridement, antibiotics, intensive care support) or standard care plus HBOT.
Some Australian hospitals have used HBOT as part of the treatment for NSTI for many years, based on early work in clostridial infections, clinical experience and several retrospective and prospective studies that indicate HBOT may provide a mortality benefit.1–3
There has not previously been an RCT addressing this. Challenges in planning an RCT are imposed by the rarity of NSTI (requiring a multicentre, international study to achieve adequate power), the practical issues and considerations for the management of severely ill patients, as well as uncertainty amongst stakeholders regarding the presence or absence of equipoise for the role of HBOT in the treatment of NSTI.
Equipoise is a state of genuine uncertainty regarding the role of a treatment modality or the superiority of one treatment over another. It is a fundamental requirement of ethical clinical research, seeking to first do no harm. Equipoise may exist in an individual clinician who is indifferent to the treatment modalities (‘individual equipoise’) or amongst the expert medical community where ‘honest professional disagreement’ exists regarding the role of a treatment, or regarding which treatment modality is best (‘clinical equipoise’).4,5 A reliance on individual equipoise of all clinician investigators in a trial, presents potentially insurmountable obstacles to the commencement or completion of a controlled trial, and the impact of such a scenario on an RCT for HBOT in NSTI will be discussed below. In contrast, clinical equipoise considers the entire range of expert medical opinion as a priori equally valuable; essentially constituting a ‘fair bet’ procedure – and as such RCTs in areas of clinical equipoise are considered to not present a risk of harm to trial participants.6
In this article I will endeavour to systematically address the concept of clinical equipoise specific to the role of HBOT in NSTI.
Commentary
The critical question is ‘is it ethical for centres which already utilise HBOT as an adjunct to standard treatment for NSTI, to be involved in a study where fifty percent of patients will be randomised to not receive HBOT? The answer involves another question (a few, actually):
IS HBOT STANDARD TREATMENT FOR NSTI?
My health service treats more cases of NSTI with HBOT per year than all other Australian and New Zealand centres combined, so this question requires particular consideration.7 To adequately answer the question, we need to review whether the provision of HBOT for NSTI is considered standard practice at the individual clinician level, Health Service level, State level, national level, and also at an international level.
IS TREATMENT OF NSTI WITH HBOT CONSISTENTLY OFFERED BY ALL CLINICIANS AT YOUR HEALTH SERVICE?
Or does the provision of HBOT depend on specific clinicians being present, rostered on, and aware of an NSTI case in your centre (e.g., an anaesthetist who is also a hyperbaric physician being made aware of the case in theatre, hyperbaric doctors ‘finding’ cases, or a ‘believer’ specialty doctor making a referral to the Hyperbaric Service)?
In centres where there is variability between clinicians, patients with NSTI are essentially already receiving ‘random’ care (e.g., receiving HBOT or not, based on factors independent of any evidence). In this case, it is roster allocations or plain chance that determine the treatment pathway the patient is allocated to, without the advantages of an RCT to advance the level of evidence for (or against) this practice. Participating in an RCT simply changes the mode of allocation of treatment that is already occurring in many centres (amongst numerous other advantages).
IS THERE A CONSENSUS AMONGST CLINICIANS AT YOUR HEALTH SERVICE ABOUT THE ROLE OF HBOT FOR NSTI?
In Melbourne, we treat more cases of NSTI with HBOT than any other centre in Australia or New Zealand.7 Despite this, there is still a lack of consensus about the role of HBOT for NSTI.
Indeed, we evaluated this specific question and published our findings in ANZ Journal of Surgery in 2021.8 We surveyed experts at our centre on their beliefs about the role of HBOT in the treatment of NSTI. Whilst some clinicians felt strongly (n = 4, 6% strongly disagreed that HBOT has a role in the treatment of NSTI and n = 8, 12% strongly agreed), the most common response (n = 31, 45%) was not being sure if HBOT has a role in the treatment of NSTI. We concluded that there is clinical equipoise at our centre regarding the role of HBOT in the treatment of NSTI, that an RCT should be considered ethical, and that further work towards increasing the level of evidence is highly necessary.
ARE PATIENTS WITH NSTI ROUTINELY OFFERED HBOT IN YOUR STATE?
In Victoria, Austraila, they are not. Results from a (currently unpublished) project in which data from the Victorian admitted episodes dataset (VAED) and the Australia and New Zealand Intensive Care Society (ANZICS) adult patient database (APD) were linked by the Centre of Victorian Data Linkage (CVDL), indicate that less than one third of NSTI patients admitted to intensive care units in Victoria receive HBOT. That means that over two-thirds of Victorians who develop NSTI are not currently being referred for or receiving HBOT. Of interest, no statistically significant difference was found in APACHE III score or predicted risk of death in the groups who went on to receive, or not receive, HBOT.
WHAT ABOUT ON A REGIONAL LEVEL? IS HBOT FOR NSTI CONSIDERED STANDARD ACROSS AUSTRALIA & NEW ZEALAND?
It is not. Table 1 contains the number of cases of NSTI who received HBOT as reported by each Hyperbaric facility around Australasia in the 2022-2023 financial year; if the Alfred’s case numbers reflect less than one third of the Victorian NSTI case load, these statistics indicate that only a very small fraction of patients from around Australasia are currently receiving HBOT for NSTI. Assuming that disease incidence is similar across Australia and New Zealand, these data indicate a greater than ten-fold variation in the use of HBOT between regions.9,10
Table 1
Cases of necrotising soft tissue infections treated with hyperbaric oxygen in Australia and New Zealand (NZ); ACT – Australian Capital Territory; NSW – New South Wales;
NT – Northern Territory; pop – population; QLD – Queensland; SA – South Australia; TAS – Tasmania; VIC – Victoria; WA – Western Australia
|
Institution |
The Alfred Hospital (VIC) |
Fiona Stanley Hospital |
Royal Hobart Hospital |
Royal Adelaide Hospital |
Prince of Wales Hospital |
Royal Brisbane & Women’s Hospital |
Wesley Hospital |
Townsville |
Royal Darwin Hospital |
North Shore Hospital Auckland |
Christ-church Hospital |
|
Cases treated4 |
27 |
5 |
3 |
1 |
6 |
1 |
0 |
1 |
0 |
2 |
0 |
|
Population6,7 |
6,766,600 |
2,855,600 |
572,700 |
1,844,600 |
8,758,600 |
5,418,500 |
251,700 |
5,223,100 |
|||
|
Cases treated per 106 pop. |
3.99 |
1.75 |
5.24 |
0.54 |
0.69 |
0.37 |
0.00 |
0.38 |
|||
WHAT ABOUT ON AN INTERNATIONAL LEVEL? IS HBOT STANDARD PRACTICE FOR NSTI INTERNATIONALLY?
It is not. The use of HBOT for NSTI varies markedly between countries.
In July 2018 the NHS England published their Clinical Commissioning Policy: Hyperbaric Oxygen Therapy for necrotising soft tissue infections (all ages).11 They concluded that there is not enough evidence to make the treatment available at this time, and funding was removed for the use of HBOT for NSTI from 1 April 2019. Likewise in the USA, only ~ 1% of NSTI cases are treated with HBOT.12
In contrast, more than one third of patients with NSTI in Denmark receive HBOT.3
DO INTERNATIONAL SCIENTIFIC SOCIETIES UNIVERSALLY RECOMMEND HBOT FOR NSTI?
The recommendations from international societies vary; some do not recommend HBOT (e.g., The American Infectious Disease Society),13 some do recommend HBOT (e.g., The European and American Societies for diving and hyperbaric medicine),14,15 and some suggest consideration of HBOT if available and not interfering with standard treatment (e.g., World Society of Emergency Surgery and the Surgical Infection Society Europe).16
WHAT DOES COCHRANE SAY?
The authors of a Cochrane review published in 2015 concluded: “This systematic review failed to locate relevant clinical evidence to support or refute the effectiveness of HBOT in the management of necrotizing fasciitis. Good quality clinical trials are needed to define the role, if any, of HBOT in the treatment of individuals with necrotizing fasciitis”.17
SO DOES CLINICAL EQUIPOISE EXIST?
Irrefutably, at every level.
Nevertheless, one could argue that with all this uncertainty, maybe it will be simpler to just stay sitting on the fence? Definitely. This trial won’t be quick, or easy. However, without a unified effort, the likelihood of completion of this RCT falls. The status quo will remain; ongoing uncertainty amongst experts, ongoing inequity for patients, and ongoing inconsistency in the delivery of care for people with NSTI at hospital, state, national and international levels.
It is critical that such an RCT is planned by experts. If a poorly planned or inadequately powered trial were to be conducted, the outcome would likely be negative and may result in reduced use of HBOT for NSTI at centres which currently utilise HBOT, regardless of the actual impact HBOT has on NSTI. Clinical opinion may also shift away from a state of equipoise, which would reduce the possibility of a future, well conducted trial.
ARE THERE ANY OTHER ETHICAL CONSIDERATIONS WE SHOULD BE THINKING ABOUT?
I think it’s important to think about the ethics of not participating in a large, well-designed, multi-national, randomised controlled trial.
Our centre could take the position that HBOT is standard practice that would be unethical to withhold from 14 of the 28 Victorian patients with NSTI we treat on average per year.
However approximately 60 other Victorians are admitted to intensive care units with NSTI each year and are not referred for HBOT, no doubt in part because the current level of evidence isn’t considered adequately robust. There are hundreds of people around Australia who develop NSTI each year who do not receive HBOT, and there will be countless other people, around the world, who will develop NSTI into the future. When deciding whether or not to participate in an RCT, we must consider the large number of people into the future who this choice will impact.
Conclusion
A carefully designed, multi-centre, international randomised controlled trial investigating whether HBOT has a mortality benefit in patients with NSTI, has the potential for profound and lasting impact regardless of the outcome. A negative study may result in reduced workload of hyperbaric units around the world, millions of healthcare dollars saved and the substantial logistics involved with transferring patients with NSTI to hyperbaric services reduced. A positive study may impact the lives of thousands of NSTI sufferers into the future by resulting in increased use of HBOT and increased survival for these patients.
Without clearer answers, health services are unlikely to invest healthcare dollars into improving capacity for hyperbaric treatment of intensive care patients (which may already contribute to the low treatment numbers currently reported in many hyperbaric centres), and many NSTI patients will not be offered HBOT as a result.
If we do nothing, and maintain the status quo, only a small fraction of NSTI cases will receive HBOT at a state, national and international level. If there is a survival benefit from HBOT – which observational data suggest may be the case - remaining at status quo will do more harm than good. Perhaps the real question should be: is it ethical not to participate?
What’s your position?
References
- Devaney B, Frawley G, Frawley L, Pilcher DV. Necrotising soft tissue infections: the effect of hyperbaric oxygen on mortality. Anaesth Intensive Care. 2015;43:685–92. doi: 10.1177/0310057X1504300604. PMID: 26603791.
- Hedetoft M, Bennett MH, Hyldegaard O. Adjunctive hyperbaric oxygen treatment for necrotising soft-tissue infections: A systematic review and meta-analysis. Diving Hyperb Med. 2021;51:34–43. doi: 10.28920/dhm51.1.34-43. PMID: 33761539. PMCID: PMC8081587.
- Hedetoft M, Madsen MB, Madsen LB, Hyldegaard O. Incidence, comorbidity and mortality in patients with necrotising soft-tissue infections 2005–2018: a Danish nationwide register-based cohort study. BMJ Open. 2020;10(10)e041302. doi: 10.1136/bmjopen-2020-041302. PMID: 33067303. PMCID: PMC7569942.
- Nardini C. The ethics of clinical trials. Ecancermedicalscience. 2014;8:387. doi: 10.3332/ecancer.2014.387. PMID: 24482672. PMCID: PMC3894239.
- Freedman B. Equipoise and the ethics of clinical research. N Engl J Med. 1987;317(3):141–5. doi: 10.1056/NEJM198707163170304. PMID: 3600702.
- Edwards SJ, Lilford RJ, Braunholtz DA, Jackson JC, Hewison J, Thornton J. Ethical issues in the design and conduct of randomised controlled trials. Health Technol Assess. 1998;2(15):i–vi, 1–132. PMID: 10194615.
- Hyperbaric Technicians and Nurses Association. Australian and New Zealand Hyperbaric Treatment Data, 1 July 2022 – 30 June 2023. HTNA 2023.
- Devaney B, Pilcher D, Mitra B, Watterson J. Does equipoise exist amongst experts regarding the role of hyperbaric oxygen treatment for necrotising soft tissue infection? ANZ J Surg. 2021;91:485–7. doi: 10.1111/ans.16337. PMID: 33847053.
- Australian Bureau of Statistics. National, state and territory population. Reference period: March 2023. [cited 2023 Oct 3]. Available from: https://www.abs.gov.au.
- Statistics New Zealand. Tatauranga Aotearoa. National population estimates: At 30 June 2023. [cited 2023 Oct 3]. Available from: https://www.stats.govt.nz.
- NHS England. Clinical Commissioning Policy: Hyperbaric Oxygen Therapy for necrotising soft tissue infections (all ages). July 2018. [cited 2023 Oct 3]. Available from: https://www.england.nhs.uk/wp-content/uploads/2018/07/hbot-for-necrotising-soft-tissue-infections-v2.pdf.
- Soh CR, Pietrobon R, Freiberger JJ, Chew ST, Rajgor D, Gandhi M, et al. Hyperbaric oxygen therapy in necrotising soft tissue infections: a study of patients in the United States Nationwide Inpatient Sample. Intensive Care Med. 2012;38:1143–51. doi: 10.1007/s00134-012-2558-4. PMID: 22527074.
- Stevens DL, Bisno AL, Chambers HF, Dellinger EP, Goldstein EJ, Gorbach SL, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the infectious diseases society of America. Clin Infect Dis. 2014;59:147–59. doi: 10.1093/cid/ciu296. PMID: 24947530.
- Mathieu D, Marroni A, Kot J. Tenth European Consensus Conference on Hyperbaric Medicine: recommendations for accepted and non-accepted clinical indications and practice of hyperbaric oxygen treatment. Diving Hyperb Med. 2017;47:24–32. doi: 10.28920/dhm47.1.24-32. PMID: 28357821. PMCID: PMC6147240.
- Moon RE, editor. Undersea and Hyperbaric Medical Society. Hyperbaric oxygen therapy indications. 14th ed. North Palm Beach (FL): Best Publishing Company; 2019.
- Sartelli M, Coccolini F, Kluger Y, Agastra E, Abu-Zidan FM, Abbas AES, et al. WSES/GAIS/WSIS/SIS-E/AAST global clinical pathways for patients with skin and soft tissue infections. World J Emerg Surg. 2022;17(1):1–23. doi: 10.1186/s13017-022-00406-2. PMID: 35033131. PMCID: PMC8761341.
- Levett D, Bennett MH, Millar I. Adjunctive hyperbaric oxygen for necrotizing fasciitis. Cochrane Database Syst Rev. 2015;1(1):CD007937. doi: 10.1002/14651858.CD007937.pub2. PMID: 25879088. PMCID: PMC6516968.
Conflicts of interest and funding: nil
Submitted: 17 November 2023
Accepted after revision: 19 January 2024
Copyright: This article is the copyright of the author who grants Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms