52 - 55












- Super User
- Category: Information
- 2506
Supplementary Table (S1) Reference List
Agadzhanian NA, Dvorzhak I, Kaliuzhnuyi LV, Moravek M. [Changes in the EEG and behavioural reactions at difference degrees of hypoxia]. Zh Vyssh Nerv Deiat Im I P Pavlova. 1971;21:176–83. PMID: 5562620.
Aleksandrov MV, Ivanov AO, Aleksandrova TV, Lutsyk MA. [Mechanisms of adaptation effect of normobaric hypoxic therapy]. Vopr Kurotol Fizioter Lech Fiz Kult. 2001;1:18–21. PMID: 11530401.
Alekseev DA, Zubarev AF, Krupina TN, Iarullin KK, Kuznets EI. [Hemo-and neurodynamics of the human brain during exposure to moderate hypoxic exposure]. Kosm Biol Aviakosm Med. 1984;18:81–6. PMID: 642367.
Baciu I, Dorofteiu M, Tomus L, Soltuz V, Derevenko P. [Effect of hypoxia on the electrical activity of the cerebral cortex and on the excitability of chemoreceptors of the carotid sinus in various modes of oxygen diffusion]. Fiziol Zh SSSR Im I M Sechenova. 1964;50:259–67. PMID: 14209883.
Balioz NV, Krivoshchekov SG. Individual typological features in the EEG of athletes after acute hypoxic treatment. Hum Physiol. 2012;38:470–7. doi: 10.1134/S0362119712050027. PMID: 23101237.
Bertha H, Lorenzonia E, Manowarda K, Lechner H. [Polygraphic studies during an aviation-medical altitude experiment]. Wien Z Nervenheilkd Grenzgeb. 1964;21:297–323. PMID: 14260445.
Burykh EA, Nesterov SV, Soroko SI, Volkov NI. [Relationships between cerebral blood flow dynamics and bioelectric activity of the human brain in experimental acute hypoxia]. Rizio Cheloveka. 2002;28:24–31. PMID: 12564219.
Burykh EA. [Relations of the EEG local and spatialtemporal spectral characteristics changes under hypoxia in humans]. Ross Riziol Zh Im I M Sechenova. 2005;91:1260–80. PMID: 16408635.
Burykh EA. [Individual specifics of oxygen consumption by the human organism in hypoxia]. Ross Riziol Zh Im I M Sechenova. 2007;93:1292–307. PMID: 18198597.
Burykh EA. Interaction between changes in local and temporalspatial spectral EEG characteristics during exposure of humans to hypoxia. Neurosci Behav Physiol. 2007;37:133–46. doi: 10.1007/s11055-007-0161-x. PMID: 17187205.
Burykh EA, Sergeeva EG. [Electrical activity of the brain and oxygen supply for cognitive-mnestic activity in humans under different degrees of hypoxia]. Fiziol Cheloveka. 2008;36:51–62. PMID: 19133537.
Burykh EA. [Changes of external respiration, brain, circulation and the EEG in acute hypoxia in the subjects with different hypoxic resistance]. Ross Fiziol Zh Im I M Sechenova. 2011;97:459–71. PMID: 21874857.
Burykh EA. Features of the Dynamics of the Human EEG Spectrum at a Constant Level of Acute Hypoxia. Neurosci Behav Physiol. 2020;50:231–8. doi: 10.1007/s11055-019-00891-0.
Chatelier G, Galban P, Gouars M, Guillermin M, Benceny C, Santucci G. [Study of tolerance time to hypoxia in pilot trainees, during the course of their aeromedical training in a pressure-lowering cabin]. Rev Corps Sante Armees Terre Mer Air. 1971;12:515–42. PMID: 4257273.
Chen Z, Zhang G, Zhou D, Cheng X, Zhu L, Fan M, et al. [Effects of acute high altitude hypoxia on EEG power in different emotional states]. Zhongguo Ying Yong Sheng Li Xue Za Zhi. 2020;36:556–61. doi: 10.12047/j.cjap.5978.2020.117. PMID: 33719257.
Decroix L, De Pauw K, Van Cutsem J, Pattyn N, Heyman E, Meeusen R. Acute cocoa flavanols intake improves cerebral hemodynamics while maintaining brain activity and cognitive performance in moderate hypoxia. Psychopharmacology (Berl). 2018;235:2597–608. doi: 10.1007/s00213-018-4952-2. PMID: 29951768.
Ding Q, Li G, Wang B, Hu M, Li J. Complexity and Topographic Analysis of EEG under Normal and Simulated High Altitude Acute Hypoxia Conditions. In: 2005 International Conference on Neural Networks and Brain. IEEE; 2005. doi: 10.1109/ICNNB.2005.1614922.
Eckert DJ, Catcheside PG, McDonald R, Adams AM, Webster KE, Hlavac MC, McEvoy RD. Sustained Hypoxia Depresses Sensory Processing of Respiratory Resistive Loads. Am J Respir Crit Care Med. 2005;172:1047–54. doi: 10.1164/rccm.200505-699OC. PMID: 15976376.
Edlinger G, Domej W, Lindner G, Pfurtscheller G, Guger C. Effects of a fast cable car ascent on the autonomic and central nervous system assessed by EEG and ECG analysis. In: Conference Proceedings. 2nd International IEEE EMBS Conference on Neural Engineering, 2005. IEEE. doi: 10.1109/CNE.2005.1419608. PMID: 17281509.
Engel GL, Webb JP, Ferris EB. Quantitative electroencephalographic studies of anoxia in humans; comparison with acute alcoholic intoxication and hypoglycemia. J Clin Invest. 1945;24:691–7. doi: 10.1172/JCI101652. PMID: 16695262. PMCID: PMC435504.
Forster HV, Soto RJ, Dempsey JA, Hosko MJ. Effect of sojourn at 4,300m altitude on electroencephalogram and visual evoked response. J Appl Aphysiol. 1975;39:109–13. doi: 10.1152/jappl.1975.39.1.109. PMID: 1150576.
Gazivoda N. [Influence of hypoxia on electroencephalographic curve]. Med Glas. 1971;25:233–7. PMID: 5148033.
Gora EP. [Effect of different regimens of voluntary respiration control on the electroencephalogram of men exposed to hypoxic hypoxia]. Kosm Biol Aviakosm Med. 1988;22:82–4. PMID: 3361845.
Guger C, Domej W, Lindner G, Edlinger G. Effects of cable car ascent to 2700 meters on mean EEG frequency and event-related desynchronization (ERD). Wien Med Wochenschr. 2005;155:143–8. doi: 10.1007/s10354-005-0161-9. PMID: 15966259.
Guger C, Krausert S, Domej W, Edlinger G, Tannheimer M. EEG, ECG and oxygen concentration changes from sea level to a simulated altitude of 4000 m and back to sea level. Neurosci Lett. 2008;442:123–7. doi: 10.1016/j.neulet.2008.06.075. PMID: 18619520.
Held K, Hohlweck P, Athanassenas G. [Effect of kallikreinon visual attention and EEG during hypoxia in man]. Med Welt. 1976;76:2323–8. PMID: 1004186.
Holmberg G. The electroencephalogram during hypoxia and hyperventilation. Electroencephalogr Clin Neurophysiol. 1953;5:371–6. doi: 10.1016/0013-4694(53)90078-9. PMID: 13068301.
Hu M, Li J, Li G, Tang X, Freeman WJ. Normal and hypoxia EEG recognition based on a chaotic olfactory model. In: Conference Proceedings. Advances in Neural Networks – ISNN 2006, 3rd International Symposium on Neural Networks, Chengdu, China. doi: 10.1007/11760191_81.
Ikeda T, Yamada S, Imada T, Matsuda H, Kazama T. Influence of hypobaric hypoxia on bispectral index and spectral entropy in volunteers. Acta Anaesthesiol Scand. 2009;53:891–4. doi: 10.1111/j.1399-6576.2009.01945.x. PMID: 19397504.
Iwama K. The influence of oxygen lack on brain waves in man. Tohoku J Exp Med. 1950;52:63–8. doi: 10.1620/tjem.52.63. PMID: 14776733.
Jernajczyk W, Sobanska A, Marczak M, Maciejewski A, Latka M, West B, Pokorski M. The influence of acute progressive hypoxia on bioelectrical activity of the brain. J Physiol Pharmacol. 2006;57:165–74. PMID: 17072043.
Kaufman D, Wesensten NJ, Pearson NR, Kamimori GH, Balkin TJ. Altitude and time of day effects on EEG spectral parameters. Physiol Behav. 1993;54:283–7. doi: 10.1016/0031-9384(93)90112-s. PMID: 8372122.
Kida M, Imai A. Cognitive performance and event-related brain potentials under under simulated high altitudes. J Appl Physiol. 1985;74:1735–41. doi: 10.1152/jappl.1993.74.4.1735. PMID: 8514690.
Konig StA, Nolle F, Ehret T, Koelfen W, Longin E, Daffertshofer M. [Comments on the mechanism of EEG changes due to hyperventilation: EEG power spectra and near-infrared spectroscopy after hyperventilation and hypoxia]. Klin Neurophysiol. 2004;35:39–44. doi: 10.1055/s-2003-814845
Kraaier V, Van Huffelen AC, Wieneke GH. Quantitative EEG changes due to hypobaric hypoxia in normal subjects. Electroencephalogr Clin Neurophysiol. 1988;69:303–12. doi: 10.1016/0013-4694(88)90002-8. PMID: 2450729.
Li G, Zhang T, Chen X, Shang C, Wang Y. Effect of intermittent hypoxic training on hypoxia tolerance based on brain functional connectivity. Physiol Meas. 2016;37:2299–316. doi: 10.1088/1361-6579/37/12/2299. PMID: 27897151.
Luft UC, Noell WK. Manifestations of brief instantaneous anoxia in man. J Appl Physiol. 1956;8:444–54. doi: 10.1152/jappl.1956.8.4.444. PMID: 13286207.
Malle C, Bourrilhon C, Quinette P, Laisney M, Eustache F, Pierard C. Physiological and cognitive effect of acute normobaric hypoxia and modulation from oxygen breathing. Aerosp Med Hum Perform. 2016;87:3–12. doi: 10.3357/AMHP.4335.2016. PMID: 26735227.
Miszczak J, Nowicki J. [Evoked average corticoauditory responses in the course of controlled hypoxia]. Otolaryngol Pol. 1975;29:343–7. PMID: 1161298.
Ozaki H, Watanabe S, Suzuki H. Topographic EEG changes due to hypobaric hypoxia at simulated high altitude. Electroencephalogr Clin Neurophysiol. 1995;94:349–56. doi: 10.1016/0013-4694(94)00311-8. PMID: 7774521.
Papadelis C, Kourtidou-Papadeli C, Bamidis PD, Maglaveras N, Pappas K. The effect of hypobaric hypoxia on multichannel EEG signal complexity. Clin Neurophysiol. 2007;118:31–52. doi: 10.1016/j.clinph.2006.09.008. PMID: 17088101.
Pokorski M, Trojecka A, Marczak M, Wierzbicka A, Jernajczyk W. Cortical activity during hypoxic hyperventilation. J Physiol Pharmacol. 2003;54:29–34. PMID: 15886408.
Prast JW, Noell WK. Indication of earlier stages of human hypoxia by electroencephalometric means. J Aviat Med. 1948;19:426–34. PMID: 18122645.
Pretorius F, Smith H, Kruger C, le Roux C, van der Linde M, Groeneveld H, Bartel P. Mild hypoxia is associated with quantitative EEG changes, but not with dissociative symptoms. S Afr J Psychiatr. 2006;12:22–5. doi: 10.4102/sajpsychiatry.v12i2.61
Ramadan MZ, Ghaleb AM, Ragab AE. Using Electroencephalography (EEG) Power Responses to Investigate the Effects of Ambient Oxygen Content, Safety Shoe Type, and Lifting Frequency on the Worker’s Activities. Biomed Res Int. 2020;2020:7956037. doi: 10.1155/2020/7956037. PMID: 32337279. PMCID: PMC7160726.
Rebuck AS, Davis C, Longmire D, Upton AR, Powles AC. Arterial oxygenation and carbon dioxide tensions in the production of hypoxic electroencephalographic changes in man. Clin Sci Mol Med. 1976;50:301–6. doi: 10.1042/cs0500301. PMID: 1261211.
Remond A, Soussen G, Lesevre N. [Effects of the inhalation of a gaseous mixture poor in oxygen (5 p. 100) on the EEG of the normal man]. Rev Neurol (Paris). 1960;102:416–22. PMID: 13740784.
Rice GM, Snider D, Drollinger S, Greil C, Bogni F, Phillips J, et al. Dry-EEG manifestations of acute and insidious hypoxia during simulated flight. Aerosp Med Hum Perform. 2019;90:92–100. doi: 10.3357/AMHP.5228.2019. PMID: 30670118.
Rozhkov VP, Soroko SI, Trifonov MI, Bekshaev SS, Burykh EA, Sergeeva EG. Cortical-Subcortical Interactions and the Regulation of the Functional State of the Brain in Acute Hypoxia in Humans. Neurosci Behav Physiol. 2009;39:417–28. doi: 10.1007/s11055-009-9160-4. PMID: 19430971.
Rozhkov VP, Trifonov MI, Soroko SI. Control the functional state of the brain based on the dynamics of integral parameters of multichannel EEG in human under acute hypoxia. Hum Physiol. 2021;41:1–13. doi: 10.1134/S0362119721010114.
Saletu B, Grunberger J. The hypoxia model in human psychopharmacology: neurophysiological and psychometric studies with aniracetam i.v. Hum Neurobiol. 1984;3:171–81. PMID: 6434496.
Saletu B, Grunberger J, Anderer P. Proof of Antihypoxidotic Properties of Tenilsetam in Man by EEG and Psychometric Analyses Under an Experimental Hypoxic Hypoxidosis. Drug Dev Res. 1987;10:135–55. doi: 10.1002/ddr.430100303.
Saletu B, Anderer P, Gruenberger J. EEG brain mapping in gerontopsychopharmacology: on protective properties of pyritinol against hypoxic hypoxidosis. Psychiatry Res. 1989;29:387–90. doi: 10.1016/0165-1781(89)90098-x. PMID: 2514439.
Saletu B, Grunberger J, Linzmayer L, Anderer P. Brain protection of nicergoline against hypoxia: EEG brain mapping and psychometry. J Nerual Transm Park Dis Dement Sect. 1990;2:305–25. doi: 10.1007/BF02252925. PMID: 2127674.
Saletu B, Grunberger J, Anderer P. On brain protection of co-dergocrine mesylate (Hydergine) against hypoxic hypoxidosis of different severity: double-blind placebo-controlled quantitative EEG and psychometric studies. Int J Clin Pharmacol Ther Toxicol. 1990;28:510–24. PMID: 2086492.
Saletu B, Grunberger J, Linzmayer L, Anderer P. Dose-response studies with co-dergocrine mesylate under hypoxia utilizing EEG mapping and psychometry. Psychopharmacology (Berl). 1992;109:30–40. doi: 10.1007/BF02245477. PMID: 1365669.
Saletu B, Schulz H, Herrmann WM, Anderer P, Shrotriya RC, Vanbrabant E. BMS-181168 for protection of the human brain against hypoxia: double-blind, placebo-controlled EEG mapping studies. Pharmacopsychiatry. 1994;27:189–97. doi: 10.1055/s-2007-1014303. PMID: 7838889.
Saletu B, Grunberger J, Anderer P, Linzmayer L, Pakesch G, Zyhlarz G. Effect-kinetics on brain protection of two codergocrine-mesylate preparations (Armexe retard and Hydergine) by EEG mapping and psychometry under hypoxia. Arch Gerontol Geriatr. 1994;18:81–99. doi: 10.1016/0167-4943(94)00533-8. PMID: 15374302.
Saletu B, Hitzenberger G, Grunberger J, Anderer P, Zyhlarz G, Linzmayer L, Rameis H. Double-blind, placebo-controlled, pharmacokinetic and – dynamic studies with 2 new formulations of piracetam (infusion and sirup) under hypoxia in man. Int J Clin Pharmacol Ther. 1995;33:249–62. PMID: 7655763.
Saletu B, Grunberger J, Anderer P, Linzmayer L. Effects of the novel neuroprotective agent, riluzole, on human brain function and behavior: II. Double-blind, placebo-controlled EEG mapping and psychometric studies under hypoxia. Methods Find Exp Clin Pharmacol. 1996;18:67–81. PMID: 8721258.
Saletu B, Grunberger J, Anderer P, Linzmayer L, Konig P. On the cerebro-protective effects of caroverine, a calcium-channel blocker and antiglutamatergic drug: double-blind, placebo-controlled, EEG mapping and psychometric studies under hypoxia. Br J Clin Pharmacol. 1996;41:89–99. doi: 10.1111/j.1365-2125.1996.tb00165.x. PMID: 8838434.
Schaffler K. [Pharmacodynamic bioequivalence of piracetam in hypoxic hypoxia]. Arzneimittelforschung. 1986;36:845–9. PMID: 3730020.
Schellart NA, Reits D. Transient and maintained changes of the spontaneous occipital EEG during acute systemic hypoxia. Avait Space Environ Med. 2001;72:462–70. PMID: 11346013.
Schneider S, Struder HK. Monitoring effects of acute hypoxia on brain cortical activity by using electromagnetic tomography. Behav Brain Res. 2009;197:476–80. doi: 10.1016/j.bbr.2008.10.020. PMID: 19000717.
Seech TR, Funke ME, Sharp RF, Light GA, Blacker KJ. Impaired Sensory Processing During Low-Oxygen Exposure: A Noninvasive Approach to Detecting Changes in Cognitive States. Front Psychiatry. 2020;11:12. doi: 10.3389/fpsyt.2020.00012. PMID: 32082202. PMCID: PMC7006237.
Shi ZY, Zhao DM, Li CM, Qian MS. Change on electroencephalogram under acute hypoxia and relationship between tolerant ability to hypoxia and adaptation ability to high altitudes. Sci Sin B. 1983;26:58–69. PMID: 6867681.
Shi Z, Zhao D, Gu Z. The influence of acute and chronic hypoxia on the electroencephalogram of human body. Sci Sin B. 1986;29:1065–76. PMID: 3576175.
Shi L, Zhang YM, Tetsuo K, Shi ZY, Fang YQ, Denoble PJ, Li YY. Simulated high altitude helium-oxygen diving. Aerosp Med Hum Perform. 2017;88:1088–93. doi: 10.3357/AMHP.4912.2017. PMID: 29157337.
Sieker HO, Wilson WP. Electroencephalographic and biochemical changes in acute hypoxia and hypercapnia. Arch Neurol. 1960;3:704–10. doi: 10.1001/archneur.1960.00450060092010.
Sokolov E, Steklova P. [Conditioned reflex to time and its course under hypoxic conditions]. Zh Vyssh Nerv Deiat Im I P Pavlova. 1970;20:1123–30. PMID: 5510106.
Soroko SI, Dimarov RM. [Individual features of the changes in bioelectric activity and hemodynamics of the human brain as affected by experimental and high-altitude hypoxia]. Fiziol Cheloveka. 1994;20:16–27. PMID: 7895987.
Soroko SI, Kurmashev RA, Dzhunusova GS. Rearrangements of the Algorithms of Interaction between Wave Components of EEGs in Subjects with Different Mechanisms of Brain Self-Regulation during Adaptation to High Altitudes. Hum Physiol. 2002;28:647–56. doi: 10.1023/A:1021187903396.
Soroko SI, Burykh EA, Bekshaev SS, Sergeeva EG. [A complex multiparameter study of the human systemic reactions to a dosed exposure to hypoxia]. Fiziol Cheloveka. 2005;31:88–109. PMID: 16250512.
Soroko SI, Bekashaev SS, Rozhkov VP. EEG markers of the disturbed systemic brain activity in hypoxia. Hum Physiol. 2007;33:546–58. doi: 10.1134/S0362119707050052.
Soroko SI, Burykh EA, Bekshaev SS, Rozhkov VP, Boiko ER. [Individual systemic reactions of human organism under acute hypoxia]. Ross Fiziol Zh Im I M Sechenova. 2012;98:1396–415. PMID: 23431769.
Tanaka S. [Influence of high altitude environment on brain function]. The Kitakanto Medical Journal. 1982;32:131–43. doi: 10.2974/kmj1951.32.131.
van der Post J, Noordzij LAW, de Kam ML, Blauw GJ, Cohen AF, van Gerven JMA. Evaluation of tests of central nervous system performance after hypoxemia for a model for cognitive impairment. J Psychopharmacol. 2002;16:337–43. doi: 10.1177/026988110201600408. PMID: 12503833.
Van der Worp HB, Kraaier V, Wieneke GH, Van Huffelen AC. Quantitative EEG during progressive hypocarbia and hypoxia. Hyperventilation-induced EEG changes reconsidered. Electroencephalogr Clin Neurophysiol. 1991;79:335–41. doi: 10.1016/0013-4694(91)90197-c. PMID: 1718705.
Wang D, Yee BJ, Wong KK, Kim JW, Dijk DJ, Duffin J, Grunstein RR. Comparing the effect of hypercapnia and hypoxia on the electroencephalogram during wakefulness. Clin Neurophysiol. 2015;126:103–9. doi: 10.1016/j.clinph.2014.04.012. PMID: 24875233.
Zani A, Tumminelli C, Proverbio AM. Electroencephalogram (EEG) alpha power as a marker of visuospatial attention orienting and suppression in normoxia and hypoxia. An exploratory study. Brain Sci. 2020;10:140. doi: 10.3390/brainsci10030140. PMID: 32121650. PMCID: PMC7139314.
Zhang T, Wang Y, Li G. Effect of intermittent hypoxic training on hypoxia tolerance based on single-channel EEG. Neurosci Lett. 2016;617:39–45. doi: 10.1016/j.neulet.2016.01.063. PMID: 26850573.
- Super User
- Category: Information
- 1071
2014-2018 SNORKELLING CASE SUMMARIES
SN1: Male, aged 25-30 years, an apparently healthy and an experienced spearfisher who was spearfishing from a remote beach with two others. After 3 hours, the wind became strong and the water rough, so they headed towards shore, the victim around 5 m behind. When the others heard a shout and looked back, they couldn’t see the victim but saw a large great white shark (GWS - Carcharodon carcharias) thrashing in the water. The victim’s body was never found although two weights and a loaded speargun with evidence of shark bites were found next day. The disabling condition (DC) was likely severe trauma.
SN2: Male, overseas tourist, aged 75-80 years, with a history of hypercholesterolaemia (rosuvastatin, aspirin) and unreported snorkelling experience. He was snorkelling with a guide in an unpatrolled area next to a jetty. There was “some chop”. After around 10 minutes, he complained of being tired so they began to return to shore with the victim lying on his back with the guide swimming next to him trying to shelter him from waves. The victim was unconscious by the time they reached shallow water and was dragged ashore by a bystander and the guide who began cardiopulmonary resuscitation (CPR). Resort staff arrived quickly and attached an automated external defibrillator (AED), but no shock was advised. Paramedics arrived soon afterwards, and, despite advanced life support (ALS), he was pronounced deceased after about 45 minutes of resuscitation. The autopsy showed congested, oedematous lungs, left ventricular hypertrophy (LVH), severe ischaemic heart disease (IHD), and mitral valve calcification. Toxicology found diphenhydramine (therapeutic). The DC was likely cardiac arrhythmia.
SN3: Female, aged 60-65 years, with a history of asthma and hypertension and an inexperienced snorkeller was snorkelling with others from the beach on reef with some swell and current. After drifting with the current, she became anxious, alerted others that she needed help and wanted to get out. She then became unconscious and cyanotic. CPR was delayed significantly from difficulty bringing the victim ashore due to the reef and conditions. The autopsy revealed intensely congested, oedematous lungs, cardiomegaly, LVH and severe IHD. The DC was likely cardiac arrhythmia.
SN4: Male, aged 50-55 years, apparently fit and healthy overseas tourist. He was an inexperienced snorkeller and was snorkelling with others from a beach in an unsupervised area next to a wharf. After complaining of swallowing water from the snorkel, he began to return towards shore, alone. He was not wearing fins. After seeing him in distress and then unconscious in water, bystanders brought him ashore and began CPR. Resort staff arrived with an AED and continued CPR until the arrival of medical professionals. Resuscitation was ceased about one hour post incident. No internal autopsy was conducted but it seems that this was likely a primary drowning.
SN5: Male, aged 55-60 years, apparently fit and healthy with unknown snorkelling experience. It is believed that he possibly went snorkelling in a very remote location, alone from a rocky platform on beach with deeper gully in a strong swell. His body was never found.
SN6: Male, aged 45-50 years, with a history of lap band surgery (no history of seizures) and unreported experience. He was snorkelling with a friend who noticed him having a seizure. The friend towed him 50 m to rocks and attempted CPR for 20 minutes before leaving him to alert emergency services. Death was reported to be due to atherosclerotic and hypertensive heart disease and it is likely the DC was cardiac arrhythmia.
SN7: Male overseas tourist, aged 70-75 years, with a history of hypertension and diabetes (enalapril, felodipine, glimepiride, metformin) was snorkelling alone from boat with an observer on deck. As he was a weak swimmer, he took a life ring for floatation. He was seen trying to submerge but had trouble due to the ring. After he did manage to submerge, he failed to resurface. He was rescued and CPR commenced but was ultimately unsuccessful despite an apparent temporary return of spontaneous circulation. The autopsy revealed mildly emphysematous lungs and severe IHD. The DC was likely cardiac arrhythmia.
SN8: Male overseas tourist, aged 70-75 years, who had not snorkelled for over five years. He had a history of hypertension, hypercholesterolaemia, reflux, back pain, all of which he failed to declare to the operator. He was snorkelling “in perfect conditions” without a buddy from a large vessel about 80 m distant and was noticed to be stationary. After being recovered by the tender, he was brought to the main vessel where CPR with supplementary oxygen was commenced. An AED was brought from other boat around 15 minutes later and, when attached, no shock was advised. The autopsy revealed congested, oedematous lungs, cardiomegaly, LVH, and moderate to severe IHD. Toxicology showed diphenhydramine and meloxicam (therapeutic). The DC was likely cardiac arrhythmia.
SN9: Female, aged 20-25 years, an overseas student who was apparently fit and healthy (with no history of seizures). She had snorkelled earlier that day with a guide and holding onto a floatation ring with others. She went snorkelling again wearing a floatation vest, suit, and fins. It was calm, with little current and good visibility. After about 20 minutes, an observer noticed that she was motionless. She was pulled onto the tender and reported to have been convulsing and with blood flowing from her mouth. When on the main vessel, CPR was commenced, an AED attached, but no shock was advised. Only an external examination was performed and there were no visible injuries. This was likely a primary drowning.
SN10: Male, aged 15-20 years, who was apparently fit and healthy and an experienced spearfisherman. He was spearfishing with four others, but two had returned to the boat when they heard the victim scream “shark”. When they pulled anchor and drove to him, they saw copious blood in the water but did not see a shark. When the victim was pulled aboard, he was initially conscious and breathing, but non-communicative and bleeding profusely from one thigh. The friends tried to control bleeding using towels, picked up the others and called emergency services. By then, the victim was unconscious and apnoeic so they began CPR. After about 30 minutes, another vessel arrived and helped with resuscitation (with supplemental oxygen and AED) and continued until the boat arrived at shore some 2 hours later, where a paramedic pronounced life extinct. The shark was believed to have been a 3.3 m tiger shark (Galeocerdo cuvier). The autopsy revealed wounds to the right hip and thigh consistent with shark bite, and laceration to the right forearm and wrist. The DC was severe trauma.
SN11: Male, aged 30-35 years, a scuba diving instructor who was also certified to free dive to 30 msw with fins and had been cleared as fit-to-dive six months earlier. He was doing extended breath-hold diving, without a buddy, from a commercial dive vessel near a group of scuba divers. He was seen to submerge and surface several times, apparently extending his breath-hold times but was then found unconscious on the seabed at a depth of 20 metres of sea water (msw). After he was brought to the surface and aboard the boat, blood and water were cleared from his airway and CPR was commenced, with the aid of supplemental oxygen and an AED. After 25 minutes, one shock was advised and given, and resuscitation continued for an hour, without success. The autopsy showed heavy, congested, oedematous lungs, cardiomegaly, and LVH. It is likely that he became unconscious from extended breath-hold and drowned. It was not reported whether he was likely to have performed pre-dive hyperventilation.
SN12: Male, aged 60-65 years, with an unknown medical and snorkelling history. He was with a friend about 300 m offshore. The sea was rough with waves of up to 2 m. The friend was standing on the reef while the victim snorkelled on the outside looking for abalone. After the friend was washed off rocks by set of large waves, the victim was no longer visible. His body washed up later about 1 km away. The autopsy report was not available, but the coroner reported that the victim had drowned.
SN13: Male, aged 55-60 years, severely obese with a history of hypertension and unreported snorkelling experience. He was snorkelling alone with some family on the beach. The family lost sight of him after 15 minutes and then found him floating face down, unconscious, and apnoeic. Nearby lifeguards were alerted and performed CPR. An AED was attached but there was no information about whether any shocks were delivered. The autopsy did not indicate “features of drowning” but revealed cardiomegaly, substantial LVH, and moderate IHD. The DC was likely cardiac arrhythmia.
SN14: Male, aged 15-20 years, fit and healthy and an experienced spearfisherman. He was spearfishing with a buddy about 25 m from rocks using a baited float trail. The water was calm and clear, and the depth was around 10 msw. A large shark (believed to have been a 4-5 m GWS) bumped the buddy and then grabbed the victim by his thigh. It then swam at the buddy who put his speargun in its mouth and fired, causing it to swim away. The buddy saw the victim facedown and lifeless and swam to beach to raise the alarm. The autopsy showed severe injury to the right thigh, frothy fluid in the mouth and trachea, and overexpanded lungs. It is likely that the victim became unconscious from the severe haemorrhaging, and subsequently drowned.
SN15: Male, aged 40-45 years, severely obese (BMI 65.4 kg.m-2), a current smoker with a history of alcohol abuse, IHD (stent) and diabetes. He was on an organised snorkel tour and was wearing a floatation aid attached by a line to the guide’s wrist. He became distressed after a short swim and, while being towed towards boat by the guide, complained of dyspnoea and became unconscious and apnoeic. The guide delivered some rescue breaths through the victim’s nose and tried to keep his head above water. It required five people to lift him into the boat, where CPR was performed by the crew and a passenger. The autopsy showed congested lungs with signs of terminal aspiration of regurgitated stomach contents, cardiomegaly, signs of previous infarct, and severe, calcified IHD. The DC was likely cardiac arrhythmia.
SN16: Male, aged 30-35 years, fit and healthy albeit with a history of steroid injections. He was an experienced spearfisherman with history of hyperventilating before breath-hold diving. He was breath-holding in swimming pool, surrounded by family and friends. He held his breath underwater for two minutes, before attempting another breath-hold about four minutes later. After three minutes, he was observed to be crouched on bottom with some bubbles coming from his mouth. After another minute, the others became concerned and pulled him from the water unconscious. CPR was commenced. Paramedics arrived quickly and implemented ALS, which was unsuccessful. The autopsy indicated hyperinflated lungs with aspiration of stomach contents, and LVH. Toxicology showed blood alcohol concentration (BAC) of 0.09%. It is likely that he drowned subsequent to apnoeic hypoxia.
SN17: Male, aged 65-70 years, an overseas tourist with no known health conditions. Apparently, he could swim but his snorkelling experience was unknown. After hiring a mask and snorkel, he set off snorkelling alone from a patrolled beach. He was found over one hour later floating face-down and unconscious around 450 m from shore, was dragged into a boat and taken ashore. Lifeguards performed CPR, an AED was attached, and it appears that at least one shock was delivered, without success. The autopsy showed congested, oedematous lungs with mild emphysematous changes, LVH and moderate IHD. This was likely a primary drowning.
SN18: Male, aged 25-30 years, an overseas tourist who was fit and healthy but an inexperienced snorkeller. He set off snorkelling with a friend in shallow, calm water in a current-prone area. The companion left and the victim continued alone, swimming into deeper water. He was later found floating face down and unconscious approximately 50 m from shore and was brought to the beach, where CPR was commenced by bystanders. A ranger arrived with an AED, but no further information was available. The autopsy revealed heavy, fluid-laden lungs, but found no primary pathology to indicate medical causation. This was likely a primary drowning.
SN19: Male, aged 15-20 years, who was fit and healthy and an experienced spearfisherman. He was spearfishing with others from a boat in water of a depth of 25 to 30 msw and using the ‘one-up-one-down’ protocol. After unsuccessfully trying to spear a fish, he collected his spear and, after a breath-hold of two minutes, he had ascended to one metre from the surface when his buddy saw him go limp and sink to the bottom. Despite multiple attempts to reach him, the others were unable to do so for almost an hour because of the depth. CPR was then attempted, unsuccessfully. The autopsy revealed petechial haemorrhages around the eyes, moderately hyperinflated, oedematous lungs, and no signs of natural disease. This drowning resulted from apnoeic hypoxia from extended breath-holding. There was no information available about whether he hyperventilated before the dive.
SN20: Male, aged 30-35 years, was snorkelling for abalone with two buddies in worsening surf conditions about 60 m from shore. He was overweighted and struggling to stay afloat. One buddy initially helped him onto some rocks and suggested he remove some weight. However, the friend was exhausted and returned to shore, last seeing the victim standing in waist-deep water. Both the victim and the buddy remaining in the water disappeared. His body was washed ashore 7 days later, still wearing the wetsuit and weight belt. The autopsy showed some decomposition and marine predation, but no signs of natural disease or trauma. This was likely a primary drowning.
SN21: Male, aged 40-45 years, who first snorkelled one week earlier. He was snorkelling for abalone with two buddies in worsening surf conditions about 60 m from shore. One friend became exhausted and returned to shore, while both divers remaining in the water disappeared. Some body parts of this victim and a wetsuit fragment were found washed up on the next day and several following days. His wetsuit was identified by family, and the body parts through DNA. It is likely that he drowned and was then predated upon by a shark.
SN22: Male, aged 75-80 years, who, although diagnosed as pre-diabetic (metformin), was reportedly reasonably fit, recently participating in a hiking trip. He was a non-swimmer and an inexperienced snorkeller. He was snorkelling solo in a roped and supervised area with a calm sea and little current. In addition to mask, snorkel, and fins, he was wearing a buoyancy vest and took a “noodle” for extra floatation. There were about 100 snorkellers under the supervision of a single lookout. Although the lookout noted that the victim hadn’t moved for possibly 20 minutes, no action was taken. However, when the victim’s wife became concerned and alerted an instructor, the victim was retrieved by tender, unconscious and apnoeic with blood-stained fluid exuding from his mouth. CPR was performed using supplemental oxygen, an AED was attached but it was unclear if any shocks were delivered. The victim was declared deceased when medical aid arrived an hour later. The autopsy revealed pulmonary congestion and oedema, cardiomegaly, LVH, and moderate IHD. This was likely a primary drowning.
SN23: Male, aged 75-80 years, an overseas tourist who was apparently fit and healthy with unknown snorkelling experience. Wearing mask, snorkel, fins, and a stinger suit, he had just entered the water from a pontoon when a lookout saw him sinking quickly. He was promptly recovered from the bottom (5 msw), unconscious, apnoeic, cyanotic, and with frothy sputum oozing from his mouth. CPR was begun within two minutes of the incident, and an AED was attached but no shock was advised. CPR was ceased after 30 minutes. The autopsy revealed tracheal and bronchial oedema, congested, oedematous lungs, cardiomegaly, LVH, moderate IHD and valvular heart disease. It is possible that he drowned secondary to a cardiac arrhythmia, and/or aspirated water on entry leading to laryngospasm and drowning.
SN24: Female, aged 45-50 years, an “average” swimmer with some snorkelling experience, the latest several weeks earlier. She had a history of rheumatoid arthritis, mixed connective tissue disease and pulmonary hypertension. Although she declared dyspnoea and heart problems on a pre-dive declaration, after questioning, she was allowed to participate on a snorkelling tour with family members and a guide. She and her buddy became caught in current on entry and she became dyspnoeic and panicked. Her buddy called for help and, with the assistance of the guide and others, tried to support her although she was soon unconscious and apnoeic. A boat arrived, she was dragged aboard, CPR was begun despite difficulties due to the very confined area, and continued during the short trip to shore. Paramedics were waiting, implemented ALS and took to her hospital, where she died. The autopsy showed heavy lungs with some adhesions and cardiomegaly. The pathologist reported the cause of death as “presumed drowning”. However, a reviewing cardiologist concluded that death likely resulted from a cardiac arrhythmia, which appears to be supported by the clinical history.
SN25: Male, aged 30-35 years, reportedly fit but with a history of epilepsy (carbamazepine, clobazam, topiramate), including a recent seizure. He was an experienced breath-hold diver who was spearfishing alone and unsupervised from a small tender anchored at fringe of reef in area known for crocodiles and sharks. He disappeared and his body was never found. The cause of his death was “undetermined”.
SN26: Male, aged 30-35 years, who was obese but otherwise healthy. He was a weak swimmer and first-time snorkeller and was snorkelling solo amongst a group of 10-15 others in a marked area, only 20 m from a pontoon with lookout. The sea was slightly choppy. After possibly 7 minutes, the lookout observed that the victim was motionless in the water (depth 1 msw). After observing him for around 2 minutes, the lookout became concerned and sent someone to check. The victim was found to be unconscious and was brought to the vessel where CPR was performed. A paramedic arrived by helicopter and declared the victim to be deceased. A paramedic arrived by helicopter and declared the victim to be deceased. The autopsy showed congested lungs with foreign material in some airways but “no evidence of water ingress”, and moderate LVH. This was likely a primary drowning.
SN27: Male, aged 55-60 years, an experienced spearfisherman with an unremarkable medical history other than varicose veins. Wearing mask, snorkel, fins, wetsuit, and weight belt and carrying a speargun, he went spearfishing with a buddy. The surface conditions were not reported but there was likely a strong wind and/or current. After several dives, he complained of chest pain but decided to continue. The boat’s anchor dragged and the victim swam to chase it, and, when trying to reboard the boat, he ditched his weights, became unconscious and drifted away from the boat. The buddy, swam to him, attempted in-water CPR, and, unable to reach the boat, was forced to abandon the victim to try to save himself. Fortunately, he was found by a passing boat, clinging to a buoy. The victim’s body was recovered later that day. The autopsy found congested, oedematous lungs, equivocal cardiomegaly, LVH, and moderate IHD. The DC was likely cardiac arrhythmia.
SN28: Male, aged 25-30 years, with a history of smoking and Methylenedioxymethamphetamine (MDMA) use and unreported snorkelling experience. After having ½ bottle of wine, two beers and an MDMA tablet, he went snorkelling with a friend from a rock platform in rough seas. The friend returned to the rocks briefly, and, after reentering the water, could no longer see the victim. Other snorkellers located him on the bottom at 15 msw depth, retrieved him and took him onto rocks where CPR was begun. Nearby lifeguards arrived with AED about 10 minutes later but resuscitation was unsuccessful. The autopsy showed congested, oedematous lungs, subarachnoid haemorrhage without inflammation. Toxicology recorded alcohol (BAC 0.07%), tetrahydrocannabinol (THC), MDMA, and ethylene. It was unclear whether the DC was asphyxia from water aspiration, or cardiac arrhythmia.
SN29: Male, aged 20-25 years, an overseas tourist who was a weak swimmer who used a ‘noodle’ for floatation in an earlier snorkel activity. He went snorkelling alone and in a separate direction to his friends in an area with a strong current and high waves. His body was found floating 700 m from his entry point many hours later. Autopsy details were unavailable, but he was reported to have drowned.
SN30: Male, aged 70-75 years, who was apparently healthy and an experienced snorkeller. Wearing mask, snorkel, and fins, he was snorkelling through a channel with a strong current when and his buddy both got into difficulties and became separated trying to swim against the current into shallower water. Rescuers found the victim floating face-down and dragged him onto their boat. He was unconscious, cyanotic, with fixed, dilated pupils and frothy sputum. CPR was commenced, complicated by water and froth in the mouth, and continued until doctor arrived and declared life extinct. The autopsy found congested, oedematous lungs, cardiomegaly, severe IHD and cardiac scarring. The DC was likely cardiac arrhythmia.
SN31: Male, aged 65-70 years, an overseas tourist with a history of hypertension (valsartan) and dyspnoea with exertion, although he was recently cleared on a pre-travel medical check. After snorkelling for 10 minutes, he indicated that he wanted to return to the boat, which he did, but collapsed 10 minutes later. CPR was commenced using supplemental oxygen, and an AED was attached and delivered 6-8 shocks, without success. No internal examination was conducted, but he likely the DC was a cardiac event.
SN32: Male, aged 25-30 years, obese with unknown medical, swimming, and snorkelling histories. Wearing mask, snorkel, fins, a wetsuit, and weight belt, he was snorkelling from shore in rough conditions collecting abalone and crabs with three friends. After aborting the dive after 10 minutes due to the conditions, the friends sighted the victim face-down in breaking waves without his mask and snorkel but were unable to reach him. His body washed ashore 30 minutes later, the friends attempted CPR briefly, but abandoned this due to lack of training. Paramedics arrived around 13/4 hours post incident and unsuccessfully attempted ALS for 30 minutes. External examination showed a superficial head wound, a postmortem computed tomography scan (PMCT) showed no obvious natural disease, some slight lung changes. This was likely a primary drowning.
SN33: Male, aged 70-75 years, an overseas tourist who was a weak swimmer, and despite having an arrhythmia six years earlier for which he took medication for one month, was reported to be healthy and medication free. Wearing a mask, snorkel, fins, and a lifejacket, he set out from the beach with family members before continuing alone after five minutes towards a platform 70 m from shore. When a person on the platform raised the alarm, the victim was dragged onto a paddleboard before being retrieved by tender, taken to shore where staff arrived with oxygen and AED. Froth and blood were scooped from his mouth, CPR was commenced, and one shock was delivered. Despite CPR by staff and an off-duty doctor for 40 minutes, the victim was pronounced deceased by the doctor from a rescue helicopter. The autopsy reported congested, oedematous lungs and only mild IHD. This was likely a primary drowning.
SN34: Male, aged 20-25 years, with a history of Attention Deficit Hyperactivity Disorder (Dextroamphetamine) and unreported snorkelling experience. He went snorkelling alone from a beach around reef with one friend remaining on the beach and another surfing nearby. When the latter returned to shore, they became concerned as they could not see the victim. Although a fin was later found, his body was never recovered.
SN35: Male, aged 35-40 years, with an unreported medical and snorkelling history. Wearing a mask, snorkel, boardshorts and a 5 kg weight belt (no wetsuit or fins), he set off to collect abalone with two friends. The sea was rough with 1 m breaking waves. He had problems immediately when swamped by a wave, panicked, called for help, held onto a friend, but lost grip and sank. The friends grabbed him from underwater, dumped his belt and dragged him onto a rock ledge. Another friend began CPR, later relieved by police and then paramedics. Despite these efforts the victim died at the scene. PMCT showed that the lungs had a ground glass appearance, but no internal autopsy was performed. This was likely a primary drowning.
SN36: Male, aged 25-30 years, reportedly healthy but with unknown snorkelling experience. He set out snorkelling with others in canal which was calm but with a 3-4 knot current. There were other swimmers in area and considerable boat traffic. The victim was not wearing fins or using any floatation aid. When his friends went ashore, he continued alone. His friends became concerned when they could no longer see him and contacted the police. Police divers found his body the following day, on the bottom at a depth of 4.5 msw and still wearing his mask and snorkel. No internal autopsy was conducted, although PMCT showed no signs of significant trauma, no natural disease, but signs of fluid inhalation. This was likely a primary drowning.
SN37: Male, aged 60-65 years, an experienced spearfisherman with a history of IDDM (insulin 3/24). He was spearfishing alone in unreported conditions. An observer on the shore initially saw him standing on rocks but when she next looked, possibly 30-40 minutes later, he was floating in an unusual position. He was dragged from the water, unconscious, apnoeic, cyanotic, and pulseless, and CPR commenced by bystanders, followed by police and paramedics, but without success. A PMCT showed partially fluid-filled cranial sinuses, trachea, bronchi, and oesophagus, as well as pulmonary oedema. Internal examination revealed frothy clear fluid in the trachea, heavy, oedematous lungs, LVH, moderate to severe IHD, and a possible dissection of the right coronary artery. The DC was likely cardiac arrhythmia followed by secondary drowning.
SN38: Male, aged 30-35 years, with an unknown medical history, an “average” swimmer who had snorkelled three time before. Wearing a mask, snorkel, shorts, and a t-shirt (no fins), he was snorkelling together with a friend who was swimming, about 100 m from shore where the depth was 4 msw and the visibility poor. He began to struggle (the friend suggested possibly from a cramp) and then sank out of sight. After an intensive search, his body was found later that night, on the seabed with his mask on and his snorkel clasped in one hand. PMCT was taken but not reported. External examination showed a frothy plume around his mouth but there was no internal examination. This was likely a primary drowning.
SN39: Male, aged 45-50 years, severely obese with a history of NIDDM (gliclazide, metformin) and unreported snorkelling experience. He entered the water to go spearfishing about 10 minutes after some friends who went swimming. There was a strong current. He was wearing a mask and snorkel and carrying a hand spear (there was no mention of fins). He was then seen to raise a hand for help but, by the time others reached him, he was face-down and unconscious in the water. He was towed to shore where CPR was commenced. A rescue chopper arrived after 30 minutes and he was taken to hospital where he was declared deceased. A PMCT showed some IHD but no significant acute changes and there was no mention of the lungs. There was no internal examination. Toxicology showed a very high level of glucose, which, although lower than the threshold where it would represent a clear independent cause of death, the pathologist suggested that it may have been a contributory factor to the drowning.
SN40: Male, aged 20-25 years, an overseas tourist who was likely an inexperienced snorkeller. He went on a day trip on a large commercial vessel with approximately 50 passengers. He had initially declared asthma on his pre-snorkelling questionnaire but then crossed it out. It was sunny and the sea calm with a slight current. He set out snorkelling with a friend, who later returned to the boat, and the victim continued alone amongst a large group in the water. The sole lookout didn’t notice a problem or that the victim was missing until the alarm was raised by the friend about one hour post entry. His body was sighted by a helicopter three hours later and recovered. There was copious froth around the mouth and nose. The autopsy revealed froth in trachea and bronchi, hyperinflated, congested, oedematous lungs, and a normal heart. This was likely a primary drowning. The coroner expressed concern about the possible lack of briefing to stay with a buddy.
SN41: Male, aged 60-65 years, an overseas tourist with unknown snorkelling experience but who was severely obese with a history of IDDM, IHD, previous coronary artery bypass surgery, and who required oxygen to walk from a plane several days earlier. He was on a day cruise on a large commercial vessel and had snorkelled for an unreported time and complained of dyspnoea and collapsed shortly after returning to the pontoon. Oxygen therapy was initially provided, but he soon deteriorated. CPR was commenced, an AED attached and, after 15 minutes, a shock was advised and delivered. CPR was continued with another six shocks delivered but was ultimately unsuccessful. Autopsy revealed heavy, oedematous lungs, cardiomegaly, LVH, and severe IHD. The CC was likely cardiac arrhythmia.
SN42: Male, aged 70-75 years, an overseas tourist who was apparently fit and healthy, albeit a history of hypertension for which medication was no longer prescribed, and who was taking aspirin daily for unreported reasons. He was an experienced snorkeller and certified scuba diver. He was snorkelling with a buddy while others from the same boat dived nearby. The sea was choppy and murky with a strong current. The buddy aborted the dive due to the current, swam back to boat, and, on boarding, saw the victim waving for help before losing sight of him. After a search for around 25 minutes, the victim was found, floating face-down and unconscious. In water rescue breathing (IWRB) was attempted before he was brought aboard the vessel where CPR was commenced. An AED, oxygen equipment, a supraglottic airway, and a mechanical chest compression device were brought from a nearby resort and utilised. One defibrillation shock was advised and delivered. A doctor arrived and pronounced the victim deceased after 50 minutes of CPR. The autopsy showed froth in the bronchi and oedematous lungs. There was some mild IHD with an otherwise normal heart. It is likely that the adverse conditions led to primary drowning.
SN43: Female, aged 35-40 years, who was currently believed to be fit and healthy. She had previously been treated for thyroid dysfunction but was no longer requiring medication. Two years earlier, tests revealed elevated blood creatine kinase levels, but this was not investigated. She was an experienced scuba instructor and the skipper of a tourist yacht. It was sunny with strong winds and the sea was choppy with a 1-metre swell and a strong current. The tender had come adrift, and dressed in a bikini, the victim entered the water wearing a mask and fins to swim to a boat about 400 m distant to use it to retrieve the tender. It is unclear if she was wearing a snorkel. The lookout watched her for some time and noted she was swimming steadily, although being pushed off course by current. The lookout then left to go to toilet and on return could no longer see the victim. A search was activated, and she was found floating face-down, without mask, about 45 minutes later. She was cyanotic with fixed, dilated pupils. Blood exuded from her mouth with the initial compressions. An AED was attached but no shock was advised. A supraglottic airway was inserted and adrenaline administered by a trainee paramedic, without success. A PMCT showed no obvious cause of death. Autopsy revealed congested, oedematous lungs, borderline cardiomegaly, and severe IHD. The DC was likely cardiac arrhythmia followed by secondary drowning.
SN44: Male, aged 75-80 years, who was severely obese and with a history of recent triple bypass surgery and emphysema, and with unreported snorkelling experience. He was on a day trip with a large snorkelling operator and failed to declare his medical status. He set off wearing mask, snorkel, fins, and a buoyancy vest but was observed motionless, face-down inside the roped off snorkel area, and brought back to the pontoon where CPR was commenced. Supplemental oxygen was administered, an AED was attached (no report of outcome) and adrenalin was administered by a bystander doctor who later pronounced the victim deceased. Autopsy revealed severe emphysema with no signs of drowning, cardiomegaly, severe ischaemic fibrosis, and severe IHD. The DC was likely cardiac arrhythmia.
SN45: Female, aged 15-20 years, who was fit and healthy but with unreported snorkelling history. She went snorkelling from a remote beach with three friends. The conditions were rough, with waves breaking onto nearby rocks and there was a strong current and rip. The group swam out approximately 15 m from shore but decided to return to shore as conditions proved more treacherous than thought. Two managed to swim to shore despite the waves and rip, while the victim and another were swept towards rocks. The victim was smashed against the rocks, from where she was recovered after 20 minutes. CPR attempts were unsuccessful. The autopsy showed a fractured dislocation of spine (C3-C4) and separation of cervical spinal cord. There was little evidence of drowning. She died after a neck dislocation.
SN46: Male, aged 70-75 years, an overseas tourist with a history of hypercholesterolaemia and anxiety but who was generally fit and ran regularly. He was a weak swimmer and inexperienced snorkeller who went snorkelling from shore with a buddy in shallow water. He indicated that he wanted to return to shore while his buddy kept snorkelling. Ten minutes later when his buddy couldn’t see him, the alarm was raised and the victim was found face-down, unconscious, and apnoeic and brought ashore. CPR was commenced by bystanders. An AED, oxygen equipment, a supraglottic airway and a mechanical chest compression device were brought from a nearby resort and utilised by staff. One defibrillation shock was advised and delivered, and a resort doctor administered adrenalin, without success. The autopsy showed congested, oedematous lungs, and a focal lesion of severe IHD. Death was from drowning, but it was unclear if this was due primarily to water aspiration or a cardiac arrhythmia.
SN47: Male, aged 40-45 years, obese and with a history of bipolar affective/schizoeffective disorder (olamzapine, diazapam). He was an experienced spearfisherman who set out spearfishing from shore with buddy wearing a mask, snorkel, fins, a wetsuit, and weight belt. There was a strong current and a low swell. After 10 minutes, he complained that he was unable to deal with the current and returned towards shore accompanied by his buddy. However, he became exhausted and then unconscious, and was dragged to shore by his buddy who began CPR, assisted by a bystander. After 30 minutes, resuscitation was abandoned due to exhaustion. The autopsy showed slightly hyperinflated, congested, oedematous lungs, LVH, and moderate IHD. Toxicology recorded olamzapine at potentially toxic levels and a therapeutic level of diazepam. Death may have resulted directly from olamzapine toxicity, or after a cardiac arrhythmia precipitated by high levels of olamzapine, followed by secondary drowning.
SN48: Male, aged 50-55 years, an overseas tourist with a history of obesity, NIDDM, hypertension, and angina (glucosidase, metformin, amlodipine, nitroglycerine) who declared that he was a good swimmer but his snorkelling experience was unreported. After failing to declare any medical conditions, he went snorkelling in a group from a large commercial vessel. In addition to a mask, snorkel, fins, he wore a wetsuit, and buoyancy jacket. A staff member saw him struggling and calling for help so entered water and swam towards him. The victim initially tried to swim towards the rescuer but then became unconscious with vomit in his mouth. He was dragged aboard a boat and CPR was commenced en route to shore. Once on shore, an AED was attached but no shock was advised, and supplemental oxygen was administered. ALS was implemented 60 minutes later when a doctor arrived on a rescue helicopter, but was unsuccessful. The autopsy found froth in the airways and congested, oedematous lungs, cardiomegaly, LVH, and mild to moderate IHD. The DC was likely cardiac arrhythmia followed by secondary drowning.
SN49: Female, aged 35-40 years, with a history of severe obesity, NIDDM, hypertension, oesophageal hernia, anxiety/depression, Asperger’s Syndrome, and seasonal asthma (amlodipine, atenolol, metoclopramide, sertraline). Three years earlier, she had been on life support for one week for a viral infection, resulting in diminished heart and lung function. She was a competent swimmer but had no snorkelling experience. After an hour of snorkelling, she was exhausted and needed help. A lifeguard was alerted by another snorkeller, and the victim was brought back to the pontoon by a lifeguard using a float. She was then placed in the recovery position and oxygen therapy administered. She was initially able to respond verbally but grey foam exuded from her mouth, she vomited and became unresponsive. CPR was commenced and an AED attached (result unreported). Adrenalin was administered by bystander doctor, but resuscitation was unsuccessful. The autopsy showed pulmonary oedema, cardiomegaly, myocardial fibrosis, and moderate IHD and the pathologist determined that death was due to myocardial fibrosis. The DC may have been cardiac arrhythmia but also could have been immersion pulmonary oedema (IPO).
SN50: Female, aged 55-60 years, severely obese with history of asthma (salbutamol) and diabetes (medication unknown) who was reported to be a poor to average swimmer. She was on a day trip on a commercial charter. She was wearing a mask, snorkel, fins, and a stinger suit and was holding two noodles for extra buoyancy. The conditions were choppy. After 10 minutes she and her buddy decided to return to the boat as she was struggling in the rough conditions. On reaching the boat, she was unable to climb out due to the boat’s rocking and became distressed and more dyspnoeic. She asked a crew member to get her “puffer” and she then took two breaths from it without any improvement. She soon became unconscious and cyanotic and was lifted onto the vessel where CPR was commenced by her buddy and a crew member. An emergency call was made, and a doctor arrived on the boat more than 30 minutes later and assisted with resuscitation. An AED was brought from another boat and attached (at least 40 minutes post arrest) and no shock was advised. Resuscitation was continued but the victim failed to respond. The autopsy showed cardiomegaly, severe LVH, moderate IHD, aortic stenosis, some evidence of water aspiration and a fatty liver. It is likely that exertion and possible aspiration triggered asthma and she was disabled by a cardiac arrhythmia.
SN51: Male, aged 60-65 years, apparently fit with no significant medical history other than obesity and hypercholestorolaemia (atorvastatin). He was a regular swimmer, but his snorkelling experience was not reported. He was on a commercial snorkelling charter with around 30 passengers. The water was calm and there was little current. There were several lookouts on the boat and some in-water guides. He entered the water wearing a mask, snorkel, fins, and wetsuit. During a post-snorkel head count it was realised that the victim was missing, a search was conducted, and he was found floating face-down on the surface with his mask on but snorkel out. He was unconscious, apnoeic, and cyanotic. Once on the vessel, CPR was commenced by passengers and crew. Supplemental oxygen was provided, and an AED attached but no shock was advised. When the rescue helicopter arrived an hour later, the doctor pronounced life extinct. The autopsy revealed heavy, congested, oedematous lungs, cardiomegaly, LVH and moderate to severe IHD. It is possible that he suffered a cardiac event and then drowned. Alternatively, he might have aspirated water through his snorkel and drowned. In either case, the lookouts failed to notice any problem.
SN52: Male, aged 20-25 years, overseas tourist who was apparently healthy but whose swimming and snorkelling skills were unreported. He was wearing a mask and snorkel (no fins) and snorkelling with three others from the shoreline of an island at a depth of around 2-3 msw. After approximately five minutes and while about 10 m from shore, he became distressed, waving and screaming before submerging. He was found underwater some five minutes later, brought to shore unconscious, apnoeic and cyanotic and CPR was commenced. Medical staff arrived 30 minutes post incident, an AED was attached but no shock was given. Adrenaline was later administered with no effect. No internal autopsy was performed, and the external examination revealed no clues to the cause of death, including no indications of a marine animal envenomation.
SN53: Male, aged 65-70 years, an overseas tourist who was a smoker with a history of diabetes and hypertension (metformin, sitagliptin, diltiazem). He was an inexperienced snorkeller of unknown swimming ability. After hiring a mask and snorkel and being shown how to put it together by his friend, they went snorkelling from the shore in a patrolled area in neck-deep water. After returning to shore for a break, they reentered the water and the friend swam further out, leaving the victim alone. Lifeguards were alerted to a snorkeller in distress and approached the victim on a rescue board. He was dyspnoeic and soon became unconscious. They brought him to shore and commenced CPR for an hour until a doctor arrived and pronounced life extinct. The autopsy revealed congested, oedematous lungs, cardiomegaly, LVH, moderate IHD, and myocardial scarring from a previous myocardial infarction. The likely DC was cardiac arrhythmia.
SN54: Male, aged 70-75 years, overseas tourist with a history of prostatic hyperplasia, reflux oesophagitis, arthritis, and hypertension (tamsulosin, omeprazole, aspirin, thomapyrin). There were recent reports of occasional dyspnoea. His snorkelling experience was unreported, but he was said to have been a weak swimmer. He was a member of a smaller tour group among a group of more than 200 passengers on a commercial reef tour. After some briefings at which he failed to declare any medical conditions, he entered the water wearing a mask, snorkel, fins, and a stinger suit. After a lookout noticed that he was snorkelling outside the designated area and blew his whistle, the victim responded and returned inside the roped area. However, shortly afterwards he was seen swimming in circles beyond the ropes and soon became motionless. When a rescuer reached him, the victim was unconscious, apnoeic, and cyanotic. The rescuer gave some rescue breaths, which were continued until they reached the pontoon. CPR was commenced, supplemental oxygen administered, and an AED attached but no shock advised. As no rescue helicopter was available, resuscitation was continued by a doctor and an ex-paramedic (both passengers) during the trip back to the mainland. On arrival, a waiting paramedic declared the victim to be deceased. The autopsy showed congested, oedematous lungs, cardiomegaly, LVH, and moderate to severe IHD. The likely DC was cardiac arrhythmia.
SN55: Male, aged 50-55 years, whose medical history was unreported but likely included hypertension as he was taking prescribed medications (amlodipine, telmisartan). He and three friends set out to collect abalone at a site where he had snorkelled before. The sea was very rough, with waves crashing over the rocky reef, a strong current, and the water was murky. One of the friends saw the victim dragged across the reef by waves before sinking. He alerted a nearby lifeguard who retrieved the victim by surf ski and transferred him to a rescue boat where CPR was commenced. The victim was taken to shore where CPR continued, an AED was attached, but no shock advised. He was transferred to hospital by ambulance where he died the next day. Autopsy details were not available, but the cause of death was given as hypoxic brain injury following drowning.
SN56: Male, aged 75-80 years, an overseas tourist with history of aortic aneurysm repair, hypertension, an hypercholesterolaemia (clopidogrel, atorvastatin) and unknown snorkelling experience. He was part of a group of 80 tourists, some of whom went snorkelling from a sand cay on coral reef. He went without a buddy but one in his group talked to him at one point as they treaded water uneventfully before separating. Sometime later, he was noticed to be floating face-down and unconscious around 15 m from shore. He was towed ashore, and CPR was commenced by some crew, later assisted by passengers who were doctors. An AED was attached but no shock advised. A supraglottic airway was inserted, and supplemental oxygen administered but resuscitation was unsuccessful. The autopsy showed congested, oedematous lungs, cardiomegaly, LVH, severe IHD, myocardial scarring, and evidence of aortic aneurysm repair. The DC was likely cardiac arrhythmia followed by secondary drowning.
SN57: Female, aged 75-80 years, an overseas tourist with a history of hypertension, breast cancer, anxiety/depression, and thyroid hormone deficiency (losartan/hydrochlorothiazide, letrozole, levothyroxine, alprazolam, citalopram). Her swimming competency and snorkelling experience were unreported. She was on a snorkelling tour aboard a commercial charter vessel which was anchored at a sandy cay. The water was choppy and there was some current and she was wearing a mask, snorkel, and fins. A lookout became concerned when she was noticed to be motionless and raised the alarm. Rescuers found the victim floating, face-down, unconscious, and apnoeic, and not wearing her mask and snorkel. White, frothy sputum was coming from her mouth. She was brought aboard the vessel where CPR was commenced, an AED attached but no shock advised. Resuscitation was ceased after 50 minutes. The autopsy revealed congested, oedematous lungs, cardiomegaly, LVH, mild to moderate IHD, valvular heart disease, and evidence of arrhythmogenic cardiomyopathy. The DC was likely cardiac arrhythmia followed by secondary drowning.
SN58: Male, aged 40-45 years, with a history of asthma but unreported swimming and snorkelling experience. He and two others were snorkelling from a boat near the mouth of a river in a 1 m swell. He was seen struggling after being swept about 50 m by a large wave. His companions swam to his assistance, and he complained about pain (the report did not specify where). He was helped to the boat and was sitting and drinking some water when he became cyanotic and unconscious. CPR was begun and continued for 30 minutes. Paramedics arrived and continued resuscitation for another 15 minutes before abandoning attempts. The autopsy showed congested, oedematous lungs, moderate to severe IHD, and a dilated right ventricle. It is possible that he experienced a cardiac event prior to, or after, aspirating water. His cause of death was “unascertained”.
SN59: Male, aged 30-35 years, with a recent history of episodes of chest pain with dyspnoea, as well as memory loss. His GP arranged an ECG, which was normal, and a referral to a neurologist, which had not yet occurred. He and a friend, who was a weak swimmer, went snorkelling from some rocks in choppy conditions. After 15-20 minutes the friend wanted to return to calmer water closer to shore and they both climbed onto the reef to walk towards shore. However, the victim then decided to swim while his friend walked. Sometime later, another snorkeller found the victim floating face down, unconscious with his mask in place but snorkel out. With the help of another person, the rescuer dragged the victim to shore where CPR was commenced by a bystander, a nurse. Paramedics arrived and continued resuscitation en route to hospital, where the victim was pronounced to be deceased. The autopsy showed congested, oedematous lungs, and focally severe IHD. The DC was likely cardiac arrhythmia followed by secondary drowning.
SN60: Male, aged 50-55 years, with a long history of mental health issues, polypharmacy abuse and seizures associated with drug withdrawal (codeine, morphine, diazepam, oxazepam, temazepam, paracetamol, quetiapine). He went snorkelling for lobsters, which was a regular occurrence. He was wearing a mask and snorkel, a wetsuit with boots, and a weight belt but it is unclear whether he had worn fins. A search was conducted when he failed to return home and his body was found lying between rocks and partly submerged. He was still wearing his weight belt. The external examination showed multiple bruises, abrasions, and lacerations but it is unclear if these occurred peri- or postmortem. Autopsy revealed minimal congestion, oedema or hyper-expansion of the lungs, LVH, and minimal IHD. Toxicology indicated codeine and morphine (supratherapeutic), several benzodiazepines (therapeutic), and quetiapine (sub-therapeutic). The cause of death was recorded as drowning but it is unclear how this occurred.
SN61: Female, aged 75-80 years, an overseas tourist described as “fit and healthy” and who was taking no medications. She was a weak swimmer of unreported snorkelling experience. She went snorkelling with a commercial operator from a large pontoon. After a briefing in her native language, she entered the water wearing mask, snorkel, fins, bathers, and a life vest. She swam further from the pontoon than did other family members. After some time, a lookout became concerned after observing the victim face-down and motionless. On entering the water and swimming to her, he found her to be unconscious with froth exuding from her mouth. She was brought onto the pontoon and CPR was commenced by staff, assisted by a passenger who was a doctor. An AED was attached but no shock advised. CPR continued for over 70 minutes until a paramedic arrived on a rescue helicopter and declared the victim to be deceased. The autopsy revealed a ruptured aorta among other injuries believed to have resulted from resuscitation attempts. The lungs were congested and oedematous, and there was evidence of cardiomegaly, LVH and severe focal IHD. The DC was likely cardiac arrhythmia followed by secondary drowning.
SN62: Male, aged 30-35 years, who was reportedly healthy and a good swimmer with some spearfishing experience. Wearing mask, snorkel, fins, a full wetsuit, a weight belt, carrying a speargun and towing a buoy, he went spearfishing from shore with a buddy. The buddy exited due to rough conditions and continued to observe the victim. However, he lost sight of the victim. Bystanders saw the victim floating face upwards in relatively shallow water. He was dragged to shore with foam coming from his mouth and nose and CPR was commenced by bystanders. A lifeguard, police then an ambulance attended but resuscitation was unsuccessful. The autopsy found no signs of natural disease but reported frothy, bloodstained fluid in the airways and moderately congested lungs. This appears to have been a primary drowning, but it is unclear whether it was subsequent to breath-holding.
SN63: Male, aged 60-65 years, an overseas tourist with history of obesity, transient ischaemic attack (clopidogrel and mirtazapine) was described as “not comfortable in the water” but had snorkelled previously. He was snorkelling from a pontoon with a buddy and guide, wearing buoyancy jacket and holding a life ring. After swallowing some water, he initially panicked, wanted to return to the pontoon but became unconscious on the way. The guide and other staff nearby performed a prompt rescue and commenced BLS with little delay. A supraglottic airway inserted, supplemental oxygen provided, and an AED was attached (unreported result). Resuscitation was unsuccessful. The autopsy showed pulmonary congestion and oedema, cardiomegaly, LVH, severe IHD, and valvular heart disease. The DC was likely cardiac arrhythmia.
SN64: Male, aged 55-60 years, an overseas tourist with history of NIDDM, who was a weak swimmer with unknown snorkelling experience. He was snorkelling separately from family members from a beach in calm, clear water. One of the companions thought that he had heard shouting but could not locate the source. The victim was later found floating face-down and unconscious 100 m from shore. He was brought ashore, and CPR initiated. Help was sought and an AED and oxygen equipment was later available but no shock was advised. The autopsy reported evidence of pulmonary congestion and aspiration, mild IHD, and toxicology indicated normal blood sugar levels. It is likely that this was a primary drowning.
SN65: Male, aged 35-40 years, who was fit and healthy and an experienced spearfisherman and underwater hockey player. He went spearfishing alone from his anchored boat at a familiar site in an area known for periodic crocodile sightings. Police became concerned when his car and boat were found late in the day and a search was commenced. His body was found two days later, submerged in water 2-3 m deep. A large (4 m) aggressive crocodile and some smaller crocodiles were seen nearby. The autopsy indicated multiple puncture wounds and lacerations consistent with bites from a large crocodile, as well as congested, oedematous and hyperinflated lungs. It is likely that he was attacked by a crocodile and subsequently drowned.
SN66: Male, aged 35-40 years with a history of exercise-induced asthma but otherwise very fit and healthy. He was a self-taught breath-hold diver who was using an apnea App to extend his breath-hold. He was practicing breath-holding in a shallow private pool, interspersing breath-holds while stationary and while swimming laps both on the surface and underwater. Closed-circuit television footage showed him to suddenly cease swimming, appear to have a seizure, and sink to the bottom at a depth of around one metre where he remained for 36 minutes. During that time a lap swimmer passed over him many times and a cleaner walked past on multiple occasions, both apparently unaware of the unfolding tragedy. He was finally pulled from the water 41 minutes after becoming unconscious, CPR was performed intermittently for 10 minutes with very slow compressions and few ventilations before paramedics arrived, found him to be asystolic and implemented ALS. Spontaneous circulation was restored after 20 minutes of ALS and the victim was transferred to hospital where he later died. No internal autopsy was performed. PMCT showed pseudo subarachnoid haemorrhage and death was reported to have resulted from hypoxic ischaemic encephalopathy in the setting of immersion. This was primary drowning subsequent to apnoeic hypoxia.
SN67: Male, aged 80-85 years, with no significant medical history, on no regular medications and of unknown experience went snorkelling with a buddy in relatively cool waters. After about five minutes he was noted to be dyspnoeic, coughing up water and struggling. His buddy towed him to shore after which he became unconscious. Lifesavers implemented CPR and an AED was attached (unreported result). No autopsy was available to review. The coroner attributed the death to drowning.
SN68: Male, aged 40-45 years, an overseas tourist with long history of epilepsy managed by medication (carbamazapine). He was a certified and experienced scuba diver, a competent snorkeller and a strong swimmer who had been scuba diving and snorkelling in previous days. Although with a tour group, he went snorkelling solo from a beach in tropical waters. He was wearing mask, snorkel and fins and carrying a camera. Others became concerned when his camera was found on the reef. His body was found several hours later. No resuscitation attempts were documented. The autopsy revealed a foam cone from the mouth and nose, congested lungs, mild to moderate IHD, and cerebral signs consistent with the history of epilepsy. Toxicology indicated the presence of carbamazapine at therapeutic levels. It is likely that he drowned after having a seizure.
SN69: Male, aged 60-65 years, who was severely obese with history of regular leg cramps but taking no regular medications. His last medical consultation was five years earlier. He and his buddy, both experienced snorkellers, set off to snorkel in a channel in choppy conditions and a strong current wearing masks and snorkels but no fins. The victim told the buddy that he was “not doing well” and they tried to swim to shore but struggled against the current. The buddy lost sight of the victim, was unable to return to shore and after a long delay was sighted and rescued. The victim’s body was found around 90 minutes later, floating face-down, apnoeic, and cyanotic. There was initial difficulty in dragging him aboard the rescue vessel due to his size. However, once aboard, CPR was commenced by resort staff and continued by a nurse and paramedics. An AED was available but was initially unable to be used as the pads would not adhere. ALS was implemented without success. The autopsy showed heavy and intensely waterlogged lungs, cardiomegaly, severe IHD and dilated cardiomyopathy. The DC was likely cardiac arrhythmia followed by secondary drowning.
SN70: Male, aged 25-30 years, who was reportedly very fit and an experienced “diver”. He went snorkelling with a buddy to catch crayfish and was wearing mask, snorkel, fins, and board shorts and carrying a catch bag. After several hours, the buddy swam to shore while the victim continued snorkelling solo. The buddy left the site and did not raise the alarm until the following day. The victim’s body was found three days later at a depth of 2 msw and with one arm wedged in a rock crevice. When police divers later arrived, they saw a wobbiegong shark predating on the body. The autopsy found evidence of shark bite, no signs of natural disease, but noted lung congestion and prominent alveolar fluid. Toxicology revealed the presence of alcohol as well as traces of methamphetamine and methadone. The cause of death was given as drowning, likely from entrapment in the rock crevice.
SN71: Male, aged 25-30 years, who was fit and healthy and an experienced spearfisherman. He was diving from a boat with a group who were participating in a larger spearfishing competition in water with a depth of 16 msw. One of his group dropped his speargun and the victim and some others did multiple breath-hold divers over around 20 minutes to search for it. The victim remained in the water after it was found and was last seen 25 m from the boat. The divers were not observing a close buddy system or the ‘one-up-one-down’ protocol. A search was commenced when it was realised that the victim was missing, and he was recovered from the ocean floor some 5-7 minutes later by one of the group using scuba for the search. His speargun was found with a fish attached. CPR was commenced when he was transferred to a sufficiently large boat and continued for an hour until they reached shore. Paramedics administered ALS, three shocks were delivered by the defibrillator and spontaneous respiration eventually returned. He was transferred to hospital but died two days later. The autopsy revealed oedematous, congested lungs, and no signs of natural disease. It is likely that he experienced apnoeic hypoxia from extended apnoea while spearing a fish, and subsequently drowned.
SN72: Male, aged 75-80 years, a judo instructor who was described as fit and active but had a history of NIDDM, hypercholesterolaemia and depression (metformin, januvia, paroxetine). Variously described as a good and a weak swimmer with unknown snorkelling experience, he was snorkelling from rocks with a friend watching from the beach. He appeared to be fine for more than 15 minutes. However, the friend then observed his snorkel to submerge on a couple of occasions before the victim rolled onto his side, apparently unconscious. He was dragged over reef to the shore where CPR was commenced by lifesavers. An AED was attached, and CPR continued, unsuccessfully. Only an autopsy summary was available and reported “fluid in the chest cavity”, signs of chronic lung disease, IHD (degree unspecified), and cardiac scarring. It was unclear whether his death resulted from primary drowning or if he was disabled by a cardiac event and subsequently drowned.
SN73: Female, aged 40-45 years, an overseas tourist with unknown medical and snorkelling history was pulled from the water unconscious after snorkelling in temperate waters from a commercial charter vessel. CPR was attempted unsuccessfully. No further details are available at the time of writing.
SN74: Male, aged 55-60 years, an international tourist with a history of cardiac arrhythmias, TIA (clopidogrel), depression and heavy smoking who was described as unfit, a poor swimmer and prone to anxiety. He had purchased a full-face snorkel mask online which was described by an experienced snorkeller as “… difficult to breathe in …”. The victim went snorkelling from a boat wearing his full-face snorkel mask, a light wetsuit, and fins. He complained that his mask leaked and found it difficult to breathe from. After he became caught in a current, he called to others on the boat for help. Rescuers entered the water and started to tow him towards the boat against the current. He was initially conscious and kicking his legs and reportedly breathing slowly and regularly, albeit with noisy expiration. After 15 minutes and nearing the boat, he was noticed to be without his mask, unconscious, with white frothy sputum. In-water rescue breathing was attempted, and the rescuers claimed that his head was never submerged during the entire rescue. The victim was dragged aboard another boat and CPR commenced. Police later arrived with an AED and oxygen equipment, but resuscitation was unsuccessful. The autopsy reported congested and oedematous lungs with blood-stained fluid in the pleural cavities, evidence of chronic lung disease, and severe IHD. The pathologist raised the possibility of IPO but suggested that a cardiac arrhythmia was more likely. A separate coroner later found that he had likely become hypoxic due to poor ventilation within his mask. The DC is unclear, but possible scenarios include primary drowning, hypoxia from a poorly ventilated mask, IPO, and cardiac arrhythmia.
SN75: Male, aged 40-45 years, with an unknown medical history and snorkelling experience, but reported to have been a weak swimmer. After having a beer, he and a buddy went snorkelling for abalone from the beach. The conditions were initially calm but then the wind became very strong, and the sea became rough. The victim was caught in a current and dragged around 200 m from shore where he was unable to stand. He called the buddy, who saw that he was exhausted and had difficulty staying afloat. After some initial difficulty, the buddy reached the victim and brought him ashore with help from bystanders. The victim was rolled onto his side and substantial water drained from his mouth. CPR was commenced by bystanders and later by ambulance paramedics, but resuscitation was unsuccessful. No internal examination was conducted. External examination showed some leg abrasions and the PMCT was unremarkable. This was likely a primary drowning.
SN76: Male, aged 15-20 years, with unknown medical and snorkelling histories but reportedly an inexperienced swimmer went snorkelling for abalone from the shore with two companions. The conditions were initially calm but then the wind became very strong, and the sea became rough. They were caught in a current and dragged around 300 m from shore where they were unable to stand. After reaching shore, the others noticed that the victim was not with them and they swam back to him and tried to assist, but he was panicking and dragged one of his friends underwater. Two nearby jet skiers came to help, and the victim was eventually dragged aboard one vessel and taken to shore where police and paramedics were waiting. ALS was performed without success. A PMCT was unremarkable, external examination showed some abrasions and there was no internal examination. This was another primary drowning.
SN77: Male, aged 40-45 years, with had a history of vasovagal syncope and reportedly low to moderate fitness, was a capable swimmer, scuba certified and an enthusiastic snorkeller with some experience. He initially set out snorkelling from a jetty with two companions but continued alone after they returned to shore. He was wearing a mask, snorkel, and fins, and carrying a camera. He was later seen holding onto a buoy about 20 m from the jetty, apparently resting. Witnesses heard him coughing and this is recorded on his camera. He removed his mask and snorkel and was next seen shortly afterwards face-down in the water. He was rescued and brought to the jetty where CPR commenced. A resort nurse arrived shortly afterwards and attached an AED which indicated that no shock was advised. ALS was implemented but was unsuccessful. The autopsy showed frothy fluids in airways, heavily waterlogged and congested lungs, mild LVH and minimal IHD. Death was likely from primary drowning although IPO was a possible DC.
SN78: Male, aged 30-35 years, who was very fit and healthy and on no regular medications. He was a strong swimmer, scuba instructor and experienced snorkeller who reportedly practiced predive hyperventilation. He set out from a popular beach to practice breath-holding wearing a mask, fins, shorts, a weight belt with 4.5 kg of weights, and carrying a video camera. Visibility was 3 m and the depth 3 msw. His buddy was troubled by the current and returned to shore while the victim stayed to do “one more dive”. The video recorded that he breath-held for 2:43 minutes before dropping the camera, presumably due to unconsciousness. He was not reported missing for almost an hour and after an unsuccessful search by police snorkellers, he was quickly located by a scuba diver. The autopsy revealed frothy fluid in the trachea and bronchi, markedly fluid-laden lungs but no signs of natural disease. Toxicology indicated a BAC of 0.02%, and dextromethorphan. It is likely that he was incapacitated from apnoeic hypoxia and subsequently drowned.
SN79: Female, aged 30-35 years, who was reportedly healthy but a poor swimmer and inexperienced snorkeller who was “scared of deep water”. Wearing a mask, snorkel and ‘rashie’, she went snorkelling with two friends from a man-made rock structure which bordered deeper water. One friend left for short time and was unable to find the victim on return. Another friend initially saw her partly submerged, before sinking. Police divers found her body several hours later. The autopsy showed frothy fluid in smaller airways, heavy, congested, oedematous lungs, and no signs of natural disease. This was likely a primary drowning.
SN80: Male, aged 60-65 years, an overseas tourist (who had arrived in Australia six hours earlier) with a history of hypertension (amlodipine) who reportedly enjoyed swimming but with unreported snorkelling experience. There was a slight wind and moderate swell. He was collecting abalone in shallow water approximately 15 m from rocks, amongst several hundred others doing the same. He was using a snorkel, but it is unclear whether he also had a mask or fins. He was wearing “business attire” with his pants rolled up. A family member watching from the rocks lost sight of the victim, but after hearing someone shout, he saw him face-down in the water, unconscious. Lifesavers brought the victim ashore and began CPR, which was unsuccessful. The autopsy showed congested, fluid-laden lungs and mild IHD. This was likely a primary drowning.
SN81: Male, aged 35-40 years, obese and with a history of gastro-oesophageal reflux (esomeprazole) but otherwise described as fit and healthy. He was a good swimmer but an inexperienced snorkeller, recently self-taught on U-tube. He went snorkelling for abalone, alone from a beach with a family member watching from shore. He wore a mask, snorkel, new long-bladed fins, a two-piece 5 mm wetsuit, a rubber freediving weight belt with two buckles and with 8.2 kg of weights, and carried a speargun and catch bag. After 20 minutes, he was seen approximately 90 m from shore swimming quickly shoreward and called for help. He appeared to reach downwards trying to remove something from his leg. He then submerged and reappeared several times for up to five minutes, and again called for help before disappearing. Rescuers located him 15-20 minutes later on the seabed ,at a depth of 3 msw. His mask, snorkel and fins were missing but he was still wearing is weight belt, which the rescuers found difficult to release. He was towed to shore, and froth and regurgitated material cleared from his airway before paramedics performed ALS, unsuccessfully. External examination showed no obvious injuries, and no internal examination was conducted. His cause of death was recorded as “unascertained” but was likely primary drowning, possibly after suffering leg cramps.
SN82: Female, aged 50-55 years, with a history of repaired patent ductus arteriosus, stroke and subsequent seizures (the last being 19 years earlier), hypertension, cardiomyopathy, angina, carotid artery bruit, asthma, and osteoporosis (carbamazepine, telmisartan, propranolol, salbutamol). She was an inexperienced snorkeller who practiced in a pool the day before the planned excursion. She had also become dyspnoeic on the beach that day and required salbutamol. Wearing mask, snorkel, and fins, she went snorkelling from the shore with a buddy and others. Shortly afterwards and about 200 m from shore, she complained of dyspnoea and wanted to return. While floating on her back and being towed towards shore, she was seen to arch back and become unconscious. She was then dragged onto a kayak and taken to shore where CPR was performed by bystander nurses and doctors. An AED from a nearby clinic was used several times without effect. The autopsy showed grossly oedematous lungs, general atherosclerosis but minimal IHD. The DC was likely cardiac arrhythmia.
SN83: Male, aged 20-25 years, an overseas working tourist with no known medical history and unknown experience. He was snorkelling from shore with a buddy when seen to become distressed and thrash around. The buddy went to help but aborted as he was a weak swimmer, was swallowing water and was endangered so he swam to shore and raised alarm. Staff returned in a tender and, after 10-15 minutes, located the submerged victim. The resort medic administered adrenaline and three shocks from an AED. The autopsy showed heavy, oedematous lungs but no signs of natural disease. Death was likely from primary drowning.
SN84: Male, aged 50-55 years, with history of IDDM and hypertension (insulin 5/24, moxonodine, perindropil, aspirin) who was described as competent and capable in the water and had previous snorkelling experience. Wearing a mask, snorkel, fins, and full length 3 mm wetsuit, he was snorkelling on sheltered reef from a boat in preparation for a whale shark encounter. While the group drifted with the current, the victim lagged, telling staff members that he had swallowed some water. He then became unconscious and apnoeic and was given IWRB on the way to the boat. CPR with supplementary oxygen was commenced on the boat and an AED attached (advice unknown). On reaching land, ALS was implemented by paramedics but was unsuccessful. The autopsy revealed fluid-laden lungs, cardiomegaly, moderate focal IHD and a shrunken pancreas. The DC was likely cardiac arrhythmia.
SN85: Male, aged 55-60 years, an overseas tourist with history of partial seizures and hypertension (clonazapine, amlodipine) but otherwise reportedly fit, albeit borderline obese. He was a strong swimmer with unknown snorkelling experience who went on a day reef trip on a large commercial vessel. Wearing a mask, snorkel, fins, and long-sleeved wetsuit, he was snorkelling alone with family watching from shore. After 10-15 minutes, he was noticed missing after and the alarm was raised. He was found floating, face-down, unconscious, and apnoeic in water 3-4 msw deep. CPR was initiated by cruise boat staff and continued by paramedics, and he was evacuated to hospital where he died two days later. At autopsy, his lungs were not fully examined but appeared well-inflated, there was mild cardiomegaly, equivocal LVH, and severe IHD. It is unclear if the DC was a seizure or cardiac arrhythmia.
SN86: Male, aged 35-40 years, a weak swimmer and inexperienced snorkeller who usually wore fins. Wearing a mask and snorkel but without fins, he was snorkelling for abalone while others watched from shore. The victim waved an arm holding a knife and a companion on the beach assumed that he needed some equipment. He entered the water and left the equipment near the victim who was now floating face-down, apparently moving and presumed to be fine. Others became concerned after the victim was had not moved for a while and he was brought to shore where CPR was attempted. The autopsy showed oedema in the trachea and sinuses, hyperinflated, heavy lungs, and moderate IHD. This appears to have been a primary drowning.
SN87: Male, aged 75-80 years, an overseas tourist with a history of IHD, hypertension, hyperlipidaemia, and depression (unspecified anticoagulant and statin, amlodipine, mirtazapine) and who was described as having a “heavy build”. He was snorkelling close to shore with family nearby in a current-prone area. After about 15 minutes, a gurgling sound was heard and the victim was seen to roll onto his back, unconscious. He was immediately dragged ashore, placed in the recovery position to clear his mouth, and CPR commenced promptly, initially by layperson and then by an off-duty doctor. An AED was attached but no shock was advised. Only a brief autopsy summary was available and reported cardiomegaly and severe IHD. The DC was likely cardiac arrhythmia.
SN88: Male, aged 70-75 years, an overseas tourist with no medical history and on no prescribed medications who was a competent swimmer but had never snorkelled before. He took a mask and snorkel (no fins) and set off snorkelling solo from a beach on a tropical island. About five minutes later, he was noticed to be floating in “an unnatural way” and some witnesses brought him ashore where CPR was commenced. An AED was attached but no shocks given. Paramedics arrived after about 35 minutes and administered ALS which was unsuccessful. Autopsy revealed congested, oedematous lungs, equivocal cardiomegaly, LVH, and severe IHD. It is unclear if he was disabled by a cardiac arrhythmia and then drowned, or if death was from primary drowning.
SN89: Male, aged 70-75 years, an overseas tourist with history of obesity, IDDM, hypertension, diabetes, angioplasty, and reduced mobility in one knee. He was a weak swimmer and an inexperienced snorkeller who had not done so for 10 years and was on a snorkel trip with a commercial operator. The staff identified him as a person to monitor closely and gave him a snorkel with a red label. Wearing a mask, snorkel, fins, buoyancy jacket, and stinger suit, he was snorkelling with his wife among larger group. The sea was calm with good visibility. Agreeing that that the current was too strong for them, the pair decided to return to the vessel. The lookout became concerned after noticing the victim to be motionless 50-80 m distant. He was retrieved in the tender and CPR commenced by boat staff. An AED was attached and, despite multiple analyses, only one shock was delivered. A doctor, who was a passenger, assisted until paramedics arrived on a rescue helicopter and the victim was pronounced deceased. The autopsy reported congested, oedematous lungs, cardiomegaly, equivocal LVH, and moderate to severe IHD. The DC was likely cardiac arrhythmia followed by secondary drowning.
SN90: Male, aged 15-20 years, an overseas tourist who was on a school trip. He was healthy but a weak swimmer and inexperienced snorkeller. Wearing a mask, snorkel, fins, rashie, and shorts, he set off from a patrolled beach to snorkel with some friends. He stopped 20 m from shore and his friends swam further out expecting him to return to shore. Some minutes later, he was found unconscious and partly submerged by a friend. Lifeguards brought him ashore and commenced CPR. An AED was attached and one shock delivered. ALS personnel arrived possibly 30 minutes post incident, but resuscitation was unsuccessful. The autopsy revealed congested, oedematous lungs and no signs of natural disease. This was likely a primary drowning.
SN 91: Male, aged 50-55 years, who was apparently fit and healthy. Wearing a mask, snorkel, fins and black full wetsuit. He set off alone to swim across a bay at a popular tourist destination when he was seen to be fatally attacked by what was reported to have been a 2.1 m Great White Shark. The autopsy showed severe lacerations to both legs and the cause of death reported as hypovolaemia.
- Super User
- Category: Information
- 4584
Appendix 1 to Risberg et al. Decompression procedures for transfer under pressure (‘TUP’) diving.
Download a PDF of the supplementary file here.
Extended description of candidate TUP tables
Note: Reference numbers correspond to the reference list in the main paper with the exception of four additional references that are listed at the end of this document.34-37
US Navy (USN)
Revision 7 of the USN Diving Manual9 was published in 2016. The manual includes decompression tables for surface-oriented diving with air and Nitrox as the breathing gas in the bottom phase and air and Oxygen as the breathing gas during decompression (“In water air/O2”). These procedures were developed for in-water rather than closed bell decompression. The diver will breathe compressed air during decompression deeper than 9 msw and oxygen at the 9 and 6 msw decompression stops. After 30 min of oxygen breathing the diver will breathe compressed air for 5 min (“air break”). A contingency procedure allows conversion to air breathing in the event of failure of oxygen delivery. A repetitive dive may take place 0-16h after the first dive (in some cases 18h if no Repetitive Group has been assigned). The tables have been developed based on a publicly available algorithm and parameter set (Thalmann E-L, VVAL7918). The Thalmann E-L algorithm is a neo-Haldanian nine-compartments model with T1/2 5-240 min exponential gas uptake and linear gas elimination. This deterministic model has been validated against a probabilistic model based on more than 3000 carefully monitored experimental dives15. The tables have been developed by the US Navy Experimental Diving Unit (NEDU) and a team of scientists with competency in decompression theory have regularly revised and expanded the decompression tables.
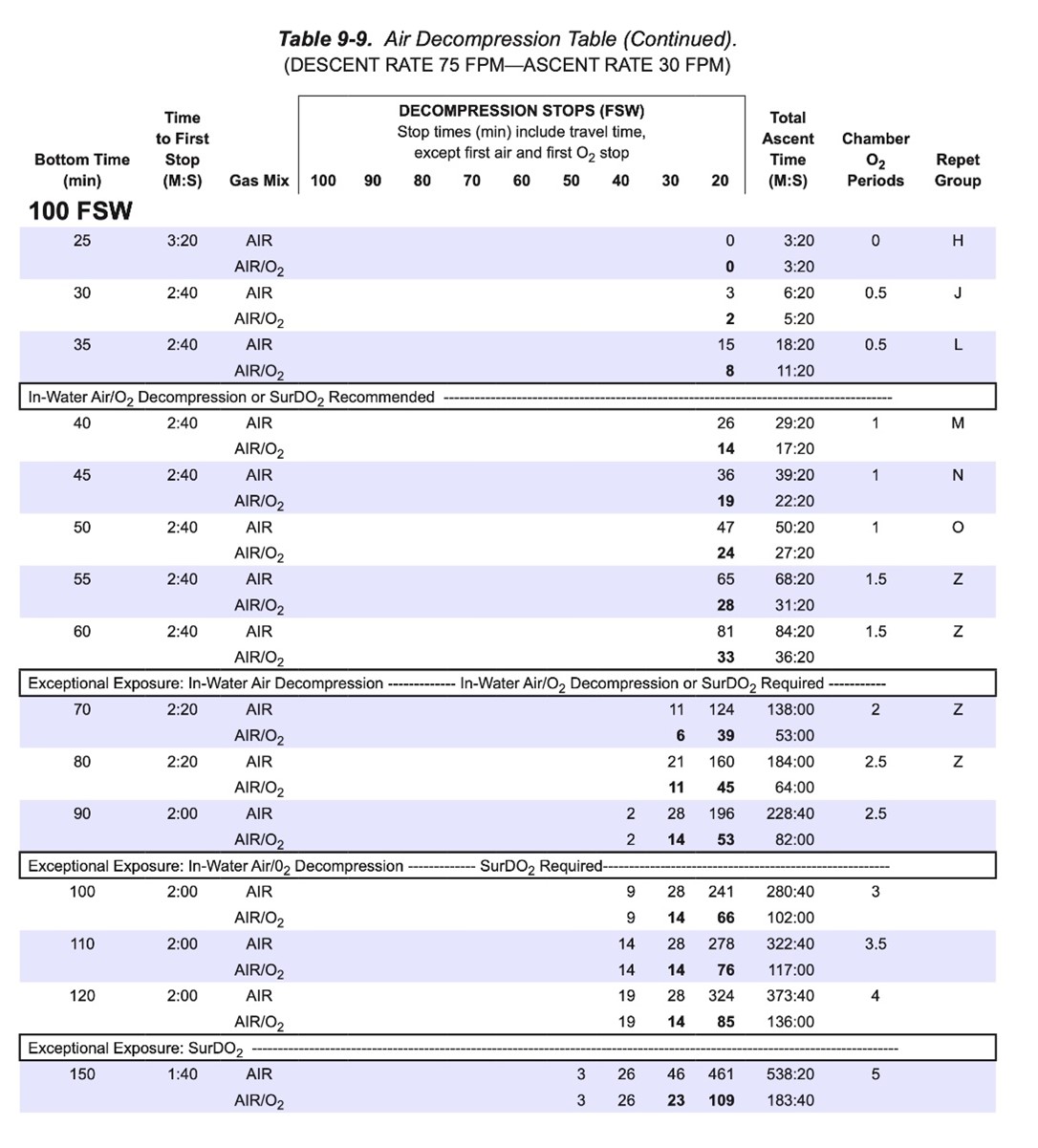
Facsimile from USN Diving Manual Rev 7 of the 100 fsw (30 msw) schedules for air and Air/O2 decompression.
MT92
The French MT 92 tables were originally published in the 1992 revision of the French diving regulations. They included a complete set of air and mixed gas tables, including Air/Standard (standard air table), Air/Oxy/6m (air tables with oxygen stop at 6msw intended for in-water decompression), Air/Oxy/12m (air tables with oxygen stop at 12 msw intended for closed bell /TUP decompression) and Air/Surface decompression. The tables came complete with nitrox, repetitive, altitude, caisson and split-level diving procedures. A contingency procedure allows conversion to air breathing in the event of a failure in oxygen delivery. The decompression for a repetitive dive is calculated based on the sum of the actual bottom time and a residual time-penalty from the preceding dive. The residual time-penalty will depend on the surface interval as well as the depth of the repetitive dive.
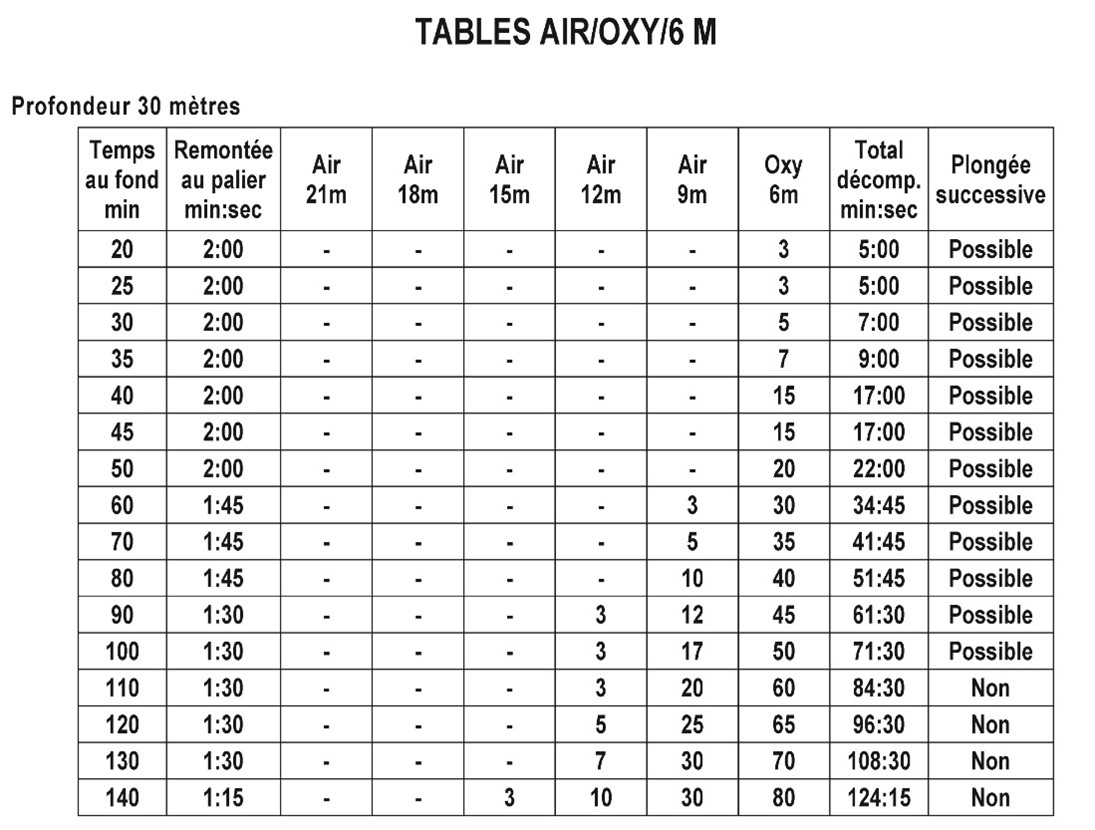
Facsimile of the MT92 “Table 5” (6 msw oxygen) for 30msw table depth.
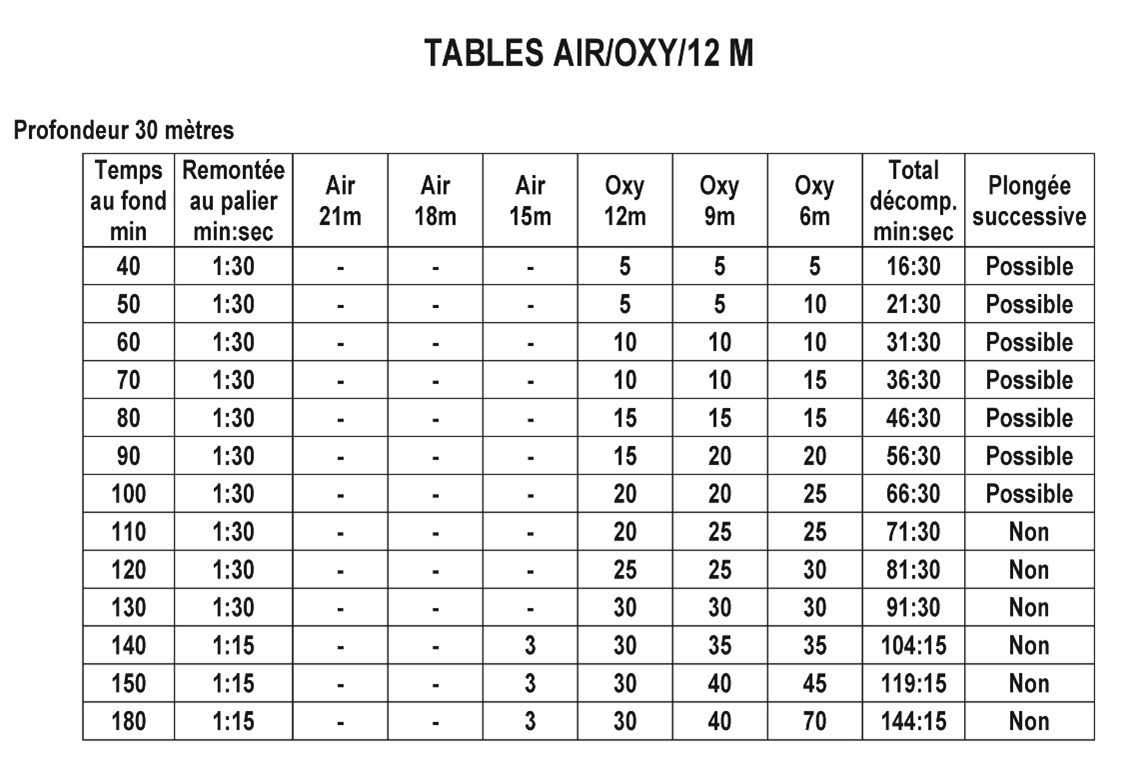
Facsimile of the MT92 “Table 6” (12 msw oxygen) for 30 msw table depth
The latest edition of the French decompression MT 92 tables was published 201211 as an annex to the diving regulations. The French tables hold two decompression procedures that may be applied for TUP-diving. One procedure (Table 5 in the original publication) was developed for open- and closed-bell decompression with Oxygen breathing 12 msw and shallower. The other procedure (Table 4 in the original publication) was developed for in-water decompression with Oxygen breathing at the shallowest 6 msw stop. Oxygen is breathed continuously without air breaks.
The MT 92 tables were initially designed by the French diving company Comex. The Comex database revealed a high DCS incidence in some subgroups of dives decompressing according to the original French 1974 tables34. In 1984 the company developed a new set of tables which was used on Comex worksites between 1986 and 1992 including a large number of air dives from surface to 51 msw on a water pipe installation in Burundi lasting a year. In 1990, these tables were presented to the French Minister of Labor who audited their validation process and reviewed their safety records before they were accepted as official procedures and included in the new diving regulations. The algorithm is a modified perfusion limited model with reduced gradients for compartments with short half times and has been described by Imbert et al.31.
Imbert has reported DCS incidence from this database for dives adhering to the 1974 tables as well as the revised tables developed 198435. From 1976 to 1983 Comex experienced a 0.3% DCS incidence in 64070 dives, but incidence reached 2.1% in the subgroup of the highest PrT index. After table revision DCS incidence was reduced to 0.1% in 33 809 dives completed during 1986-1990. The subgroup with highest PrT reached 0.9% DCS incidence.
DCIEM
The Canadian tables were issued for the first time in 1986 by the Defence and Civil Institute of Environmental Medicine (DCIEM). The latest edition was published in 2009 by Defence R&D Canada10. The tables include procedures for in-water decompression with oxygen breathing. The diver will breathe compressed air at decompression stops 12 msw and deeper, while oxygen is breathed at the shallowest 9 msw stop. A 5 min air break is recommended after 30 min of oxygen breathing. In the event of failure in oxygen provision, the decompression will be changed into a conventional air-decompression procedure. The Canadian tables allow for repetitive diving. The first dive will be awarded a “Repetitive Group”. This Repetitive Group will be converted to a numerical repetitive factor dependent on the surface interval. The equivalent bottom time for a repetitive dive is calculated by multiplying the actual bottom time with the repetitive factor. The principle is similar, but not identical, to the US Navy Diving Manual.
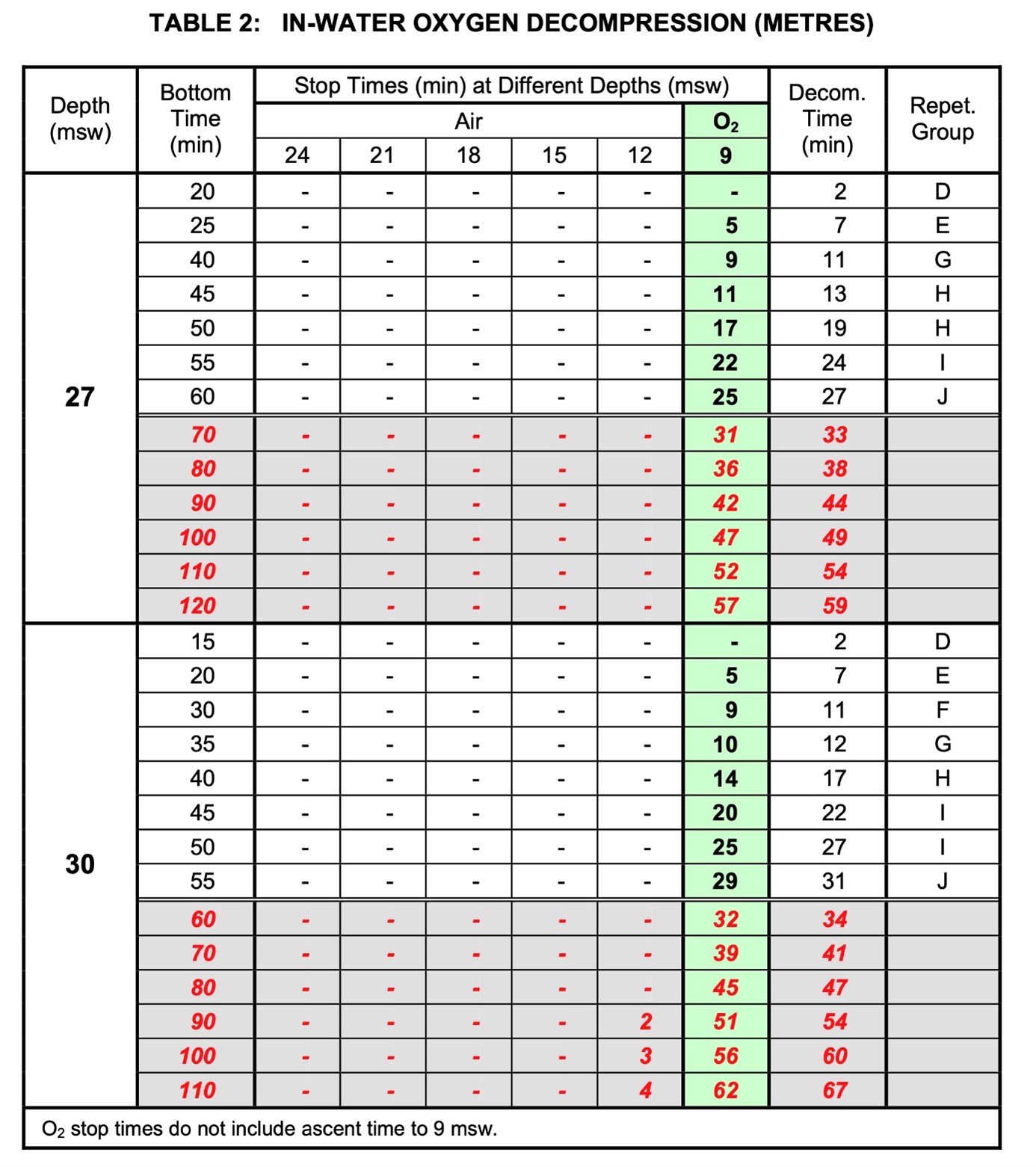
Facsimile from the DCIEM “Table 2” in-water oxygen decompression procedure. 27 and 30 msw table depth
The algorithm has been described in general terms10 and is based on diffusion-limited gas exchange with four serial compartments. The details and parameter set has not been published in public. The Canadian tables have been tested under carefully controlled conditions, including ultrasound surveillance for venous gas embolism. There is no data available to ascertain the extent these tables have been tested using oxygen as the decompression breathing gas.
DCD
The Dutch tables were last time published in 2015 by NDC and are commonly termed the DCD decompression tables12. They are based on an algorithm developed since 1975. The first air decompression tables were published by Vriens Diving and were termed the Vriens-Sterk decompression tables. In 1988, the Netherlands Diving Centre (NDC) asked Sterk to develop the NDC decompression tables, which were published in 1988 and were based on the Vriens-Sterk tables. The 1988 NDC decompression tables were only available in Dutch language. According to the author, the algorithm is a «Neo-Haldanian» sixteen-compartments model with half-times ranging 5-640 min36 (Wouter Sterk, personal communication January 2023), but neither the algorithm nor the parameters have been published in the public domain. The author reported in 1991 that more than 5000 dives completed according to these tables had been registered in a database37. The tables are officially recognized in The Netherlands and are commonly used on the Dutch continental shelf as well as abroad. We have not been able to find data on the use and experience of in-water oxygen decompression. We have included two sets of tables from DCD in our review. The first set are tables designed for wet bell decompression though they can be applied for dry bell decompression as well (Wouter Sterk, personal communication January 2023). The diver breathes oxygen at 9 and 6 msw. A five min air break is recommended after 20 min of oxygen breathing. A new single dive is allowed after a 12 h surface interval. A repetitive dive with air decompression or surface decompression with oxygen is allowed after 2-4 h. These tables have been published in public.
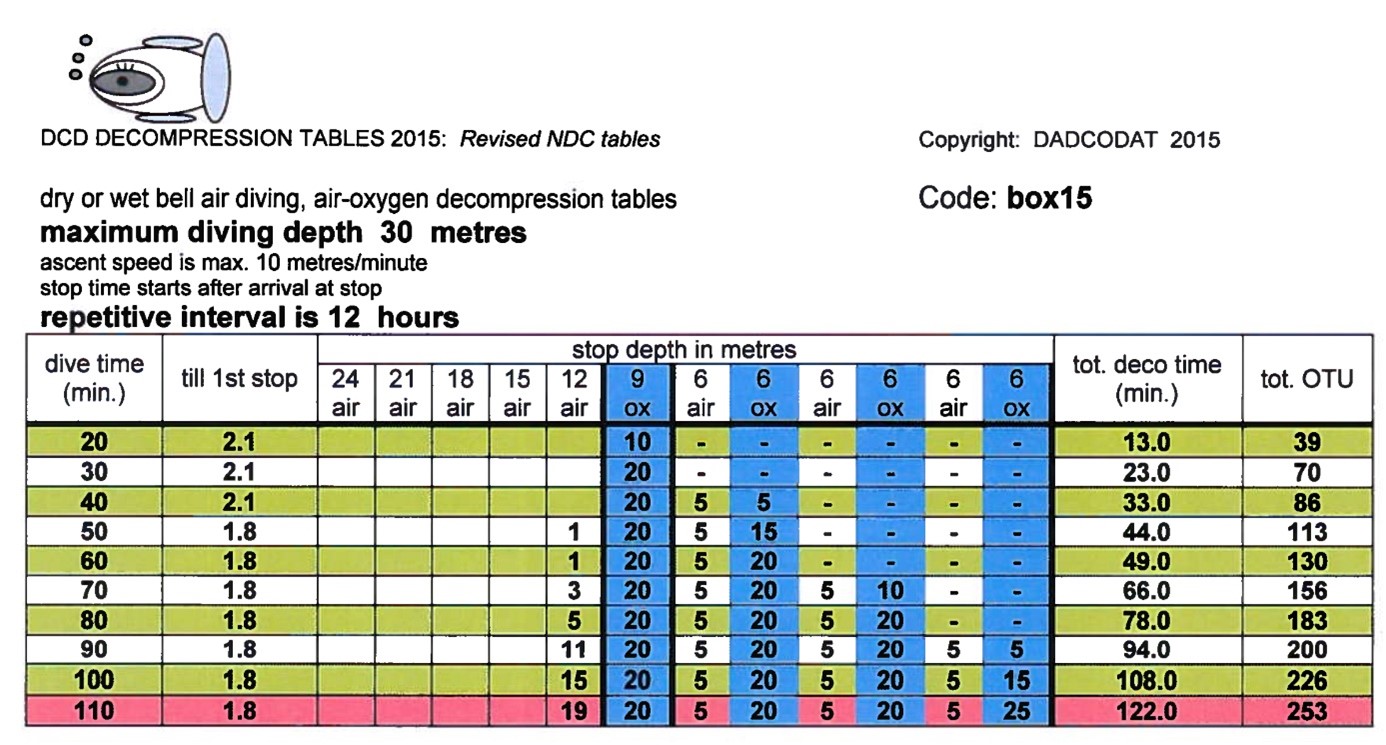
Facsimile from the DCD dry or wet bell decompression procedure. 30 msw table depth. Permission for reproduction Prof Wouter Sterk
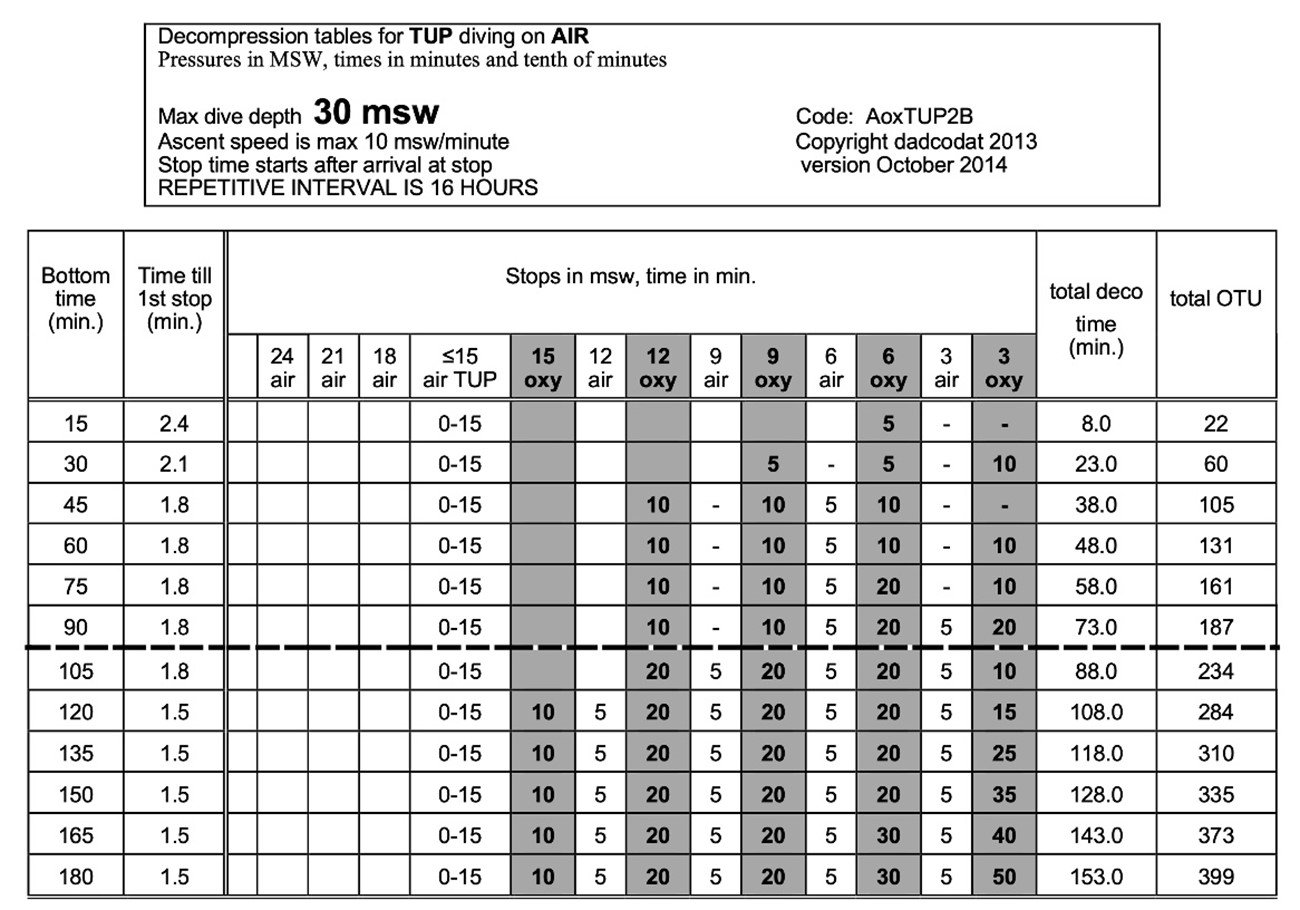
Facsimile from the DCD TUP decomperssion procedure. 30 msw table depth. Permission for reproduction Prof Wouter Sterk
The DCD AoxTUP2B TUP tables (DCD TUP tables) are not published in public but have been developed for the Dutch diving contractor N-Sea by Prof Wouter Sterk. The tables are modification of decompression tables originally developed for caisson work (Wouter Sterk, personal communication, January 2023). The tables range depths from 12 to 51 msw with the diver breathing air as the bottom gas. Compressed air is breathed on decompression stops (3 msw steps) from 24 to 18 msw. The tables are designed to allow the divers 15 min transfer time from the bell to the decompression chamber breathing air. Decompression stops at 15 msw and shallower are planned with oxygen breathing. The shallowest decompression stop is either 6 or 3 msw. A five min air break is planned after every 20 (6 and 9 msw stop) or 10 (15 msw stop) of oxygen breathing. No air break is scheduled during oxygen breathing at 3 msw.
Subsea 7 and Technip
The offshore diving contractors Subsea 7 and Technip submitted their procedures for review. Both companies use MT92 procedures as the basis for their internal procedures. Air breaks have been introduced during oxygen breathing. Random comparisons between the original MT92 tables and the company’s internal procedures disclosed differences in total decompression time in the order of 1-2 min. We consider such differences to be without practical importance and have therefore decided not to use these tables in the comparison.
Additional references
- Imbert JP, Montbarbon S. Use of the Comex diving data base. EUBS Workshop on operational dives and decompression data: collection and analysis; Amsterdam1990.
- Imbert JP. Decompression tables versus decompression procedures: an analysis of decompression sickness using diving data bases. EUBS annual meeting Heraklion, Greece. EUBS; 1991. p. 223–31.
- Sterk W. "SOX" Surface decompression tables in the eastern Scheldt. EUBS annual meeting Rotterdam, The Netherlands. EUBS; 1986. p. 115–23.
- Sterk W. The Netherlands national diving center data base. In: Sterk W, Hamilton RW, editors. EUBS Workshop. Amsterdam, The Netherlands: EUBS; 1990. p. 3–6.
- Super User
- Category: Information
- 196
Meehan, et al. Determining best practice for technical assessment of hookah surface supply diving equipment during diving fatality investigation
Appendix 1. Hookah accident data collection checklist
|
Name of deceased: Age: |
|
Training and experience: |
|
Time and Date of incident: (24hr : yyyy/mm/dd) |
|
Location of incident: |
|
Location of equipment: |
|
Date of inspection of equipment: |
|
Equipment inspected by other agencies: Y N |
|
If above Y, inspected by whom: |
|
Equipment photographed by other agencies: Y N |
|
If above Y, photographed by whom: |
|
Equipment photographed by other agencies: Y N |
|
If above Y, photographed by whom: |
|
Weather Conditions: |
|
Wind Direction at time of incident (if known): |
|
Air Inlet upwind / downwind of compressor unit: |
|
Hookah location at time of incident: Boat Flotation device Land |
|
Surface type compressor was located on (if on land) |
|
Clearance space around compressor (m): |
|
Hookah Brand: |
|
Serial Number: |
|
Description of complete system from air intake to diver(s) regulator(s): |
|
|
General overview of complete hookah system
|
Condition: |
Good |
Fair |
Poor |
Notes/Observations |
|
Air Intake Filter |
|
|
|
|
|
Air Intake
|
|
|
|
|
|
Compressor |
|
|
|
|
|
Linkage between motor and compressor (e.g., belt) |
|
|
|
|
|
Compressor motor |
|
|
|
|
|
Exhaust
|
|
|
|
|
|
Air Reserve Tank including volume |
|
|
|
|
|
Supply Hose
|
|
|
|
|
|
Hose attachments to compressor |
|
|
|
|
|
Regulator and attachment to diver
|
|
|
|
|
|
Harness/Vest |
|
|
|
|
|
Weight belt or vest |
|
|
|
|
|
Compressor Brand / Model No. |
|
Compressor motor type: Petrol Diesel Electric |
|
Engine type: 2 STROKE / 4 STROKE |
|
Fuel level: |
|
Compressed gas output: AIR NITROX |
|
Stated output in litres per minute / cubic feet per minute (CFPM): |
|
Stated line pressure (bar): |
|
Presence of a governor: |
|
Last documented service date: |
|
Inspection / Maintenance Log available: Y N |
|
Owner air test result available: Y N |
|
If Y, results: |
|
Air delivery system: Diaphragm Piston |
|
Pressure relief valve: Functioning? Y / N Setting (bar): |
|
Oil filter: Oil level: |
|
Lubricant type for internal parts (air side): |
|
Condensation drain condition: Water present in drain: Y / N |
|
Site of air hose connections relative to compressor: To reserve tank: Direct connection to compressor: |
|
Length of air intake (m): |
|
Horizontal distance of intake from compressor (m): |
|
Height of intake above compressor (m): |
|
Air intake free of obstructing debris? Y / N |
|
Air intake free of damage? Y / N |
|
Filter present at intake: Condition of filter: |
|
Filter type: Date of last change (if known): |
|
Connection type to compressor: Bayonet? Y / N |
|
Condition of exhaust port: |
|
Distance from air inlet (m): |
Air Reserve Tank
|
Storage Capacity (L): |
|
Integrated into frame of compressor or separate stand-alone unit: |
|
Construction material: Stainless Steel / Aluminium / Other (please specify): |
|
Water trap: Y / N |
|
Particle filter: Y / N Rated to (µm): |
|
Location of particle filter: Between compressor and reserve tank Between reserve tank and diver |
|
Type of particle filter: Macro particle / Carbon filter / Other (e.g. Hopcalite) |
|
Air redundancy? Yes, via surface cylinder Yes, with diver No |
Air Supply Hose
|
No. of hoses: |
|
No. of connections directly to compressor: |
|
Hose brand: |
|
Colour of hose: |
|
Condition of hose: |
|
Any visible damage / scuffs? |
|
Can hose be kinked? |
|
Length of hose (m): Internal Diameter of hose (mm): |
|
Non return valve: Present Absent |
Regulator
|
Hookah specific regulator: Y / N |
|
Modified SCUBA regulator: Y / N |
|
Brand / Model no: |
|
Condition of regulator including mouthpiece and exhalation valves: |
|
Cracking pressure of regulator: |
|
Accessory air supply: Spare Air / Octopus + Cylinder / None |
Harness / Weight Belt
|
Air Test Kit Product: |
|||
| Maximum (ppm) | Recorded (ppm) | Remarks: | |
|
Carbon Dioxide |
PASS / FAIL | ||
|
Carbon Monoxide |
PASS / FAIL | ||
|
Water Vapour |
PASS / FAIL | ||
|
Oil in air |
PASS / FAIL | ||
|
Odour |
PASS / FAIL | ||
|
Oxygen concentration (%) |
|||
|
Tested volume output of the hookah apparatus (l/min) |
|
|
Volume of reserve air tanks (l) |
|
|
(A) Maximum flow at hookah air outlet source |
|
|
(B) Maximum flow (l/min) at delivery point to regulator (1) |
|
|
(C) Maximum flow (l/min) at delivery point to regulator (2) |
|
|
Does (B) + (C) equal measurement (A) or is output flow reduced? |
|
|
Hose configuration: Is there a “Y” or “T” configuration which creates more than one air supply hose from a single outlet at the hookah apparatus? |
|
| Can steal of air be demonstrated if one regulator free flows at a shallow depth? – breathing pressure test | |
|
Driving pressure test: Differential pressure readings between surface and end of air supply hose (psi) |
0m: 5m: 10m: 15m: |
|
Time to depletion of air supply in event of compressor failure or purge of second line. |
|