52 - 55












- Super User
- Category: Information
- 17639
2023 September;53(3)
Diving Hyperb Med. 2023 September 30;53(3):172−180. doi: 10.28920/dhm53.3.172-180. PMID: 37718290. PMCID: PMC10597601.
Delivering manual cardiopulmonary resuscitation (CPR) in a diving bell: an analysis of head-to-chest and knee-to-chest compression techniques
Graham Johnson1,2, Philip Bryson3, Nicholas Tilbury1, Benjamin McGregor4, Alistair Wesson4, Gareth D Hughes1, Gareth R Hughes1, Andrew Tabner1,2
1 University Hospitals of Derby and Burton NHS Foundation Trust, Royal Derby Hospital, Derby, UK
2 University of Nottingham Medical School, East Block, Lenton, Nottingham, UK
3 International SOS, Forest Grove House, Forrester Hill Road, Aberdeen, UK
4 No specified affiliation
Corresponding author: Dr Graham Johnson, University Hospitals of Derby and Burton NHS Foundation Trust, Royal Derby Hospital, Uttoxeter Road, Derby, DE22 3NE, UK
ORCiD ID: 0000-0001-6004-6244
Keywords
Cardiovascular; Deaths; Diving deaths; Diving incidents; Diving medicine; Diving research; Resuscitation
Abstract
(Johnson G, Bryson P, Tilbury N, McGregor B, Wesson A, Hughes GD, Hughes GR, Tabner A. Delivering manual cardiopulmonary resuscitation (CPR) in a diving bell; an analysis of head-to-chest and knee-to-chest compression techniques. Diving and Hyperbaric Medicine. 2023 September 30;53(3):172−180. doi: 10.28920/dhm53.3.172-180. PMID: 37718290. PMCID: PMC10597601.)
Introduction: Chest compression often cannot be administered using conventional techniques in a diving bell. Multiple alternative techniques are taught, including head-to-chest and both prone and seated knee-to-chest compressions, but there are no supporting efficacy data. This study evaluated the efficacy, safety and sustainability of these techniques.
Methods: Chest compressions were delivered by a team of expert cardiopulmonary resuscitation (CPR) providers. The primary outcome was proportion of chest compressions delivered to target depth compared to conventional CPR. Techniques found to be safe and potentially effective by the study team were further trialled by 20 emergency department staff members.
Results: Expert providers delivered a median of 98% (interquartile range [IQR] 1.5%) of chest compressions to the target depth using conventional CPR. Only 32% (IQR 60.8%) of head-to-chest compressions were delivered to depth; evaluation of the technique was abandoned due to adverse effects. No study team member could register sustained compression outputs using prone knee-to-chest compressions. Seated knee-to-chest were delivered to depth 12% (IQR 49%) of the time; some compression providers delivered > 90% of compressions to depth.
Conclusions: Head-to-chest compressions have limited efficacy and cause harm to providers; they should not be taught or used. Prone knee-to-chest compressions are ineffective. Seated knee-to-chest compressions have poor overall efficacy but some providers deliver them well. Further research is required to establish whether this technique is feasible, effective and sustainable in a diving bell setting, and whether it can be taught and improved with practise.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Full article available here.
Diving Hyperb Med. 2023 September 30;53(3):181−188. doi: 10.28920/dhm53.3.181-188. PMID: 37718291. PMCID: PMC10597600.
An evaluation of the NUI Compact Chest Compression Device (NCCD), a mechanical CPR device suitable for use in the saturation diving environment
Andrew Tabner1,2, Philip Bryson3, Nicholas Tilbury1, Benjamin McGregor4, Alistair Wesson4, Gareth R Hughes1, Gareth D Hughes1, Graham Johnson1,2
1 University Hospitals of Derby and Burton NHS Foundation Trust, Royal Derby Hospital, Derby, UK
2 University of Nottingham Medical School, East Block, Lenton, Nottingham, UK
3 International SOS, Forest Grove House, Forrester Hill Road, Aberdeen, UK
4 No specified affiliation
Corresponding author: Dr Andrew Tabner, University Hospitals of Derby and Burton NHS Foundation Trust, Royal Derby Hospital, Uttoxeter Road, Derby, DE22 3NE, UK
ORCiD ID: 0000-0003-4191-9024
Keywords
Cardiovascular; Deaths; Diving deaths; Diving incidents; Diving medicine; Diving research; Resuscitation
Abstract
(Tabner A, Bryson P, Tilbury N, McGregor B, Wesson A, Hughes GR, Hughes GD, Johnson G. An evaluation of the NUI Compact Chest Compression Device (NCCD), a mechanical CPR device suitable for use in the saturation diving environment. Diving and Hyperbaric Medicine. 2023 September 30;53(3):181−188. doi: 10.28920/dhm53.3.181-188. PMID: 37718291. PMCID: PMC10597600.)
Introduction: Provision of manual chest compressions in a diving bell using a conventional technique is often impossible, and alternative techniques are poorly evidenced in terms of efficacy and sustainability. The first mechanical cardiopulmonary resuscitation (CPR) device suitable for use in this environment, the NUI Compact Chest Compression Device (NCCD), has recently been designed and manufactured. This study assessed both the efficacy of the device in delivering chest compressions to both prone and seated manikins, and the ability of novice users to apply and operate it.
Methods: Compression efficacy was assessed using a Resusi Anne QCPR intelligent manikin, and the primary outcome was the proportion of compressions delivered to target depth (50–60 mm). The gold standard was that achieved by expert CPR providers delivering manual CPR; the LUCAS 3 mCPR device was a further comparator.
Results: The NCCD delivered 100% of compressions to target depth compared to 98% for the gold standard (interquartile range 1.5%) and 98% for the LUCAS 3 when applied to both supine and seated manikins. The NCCD sometimes became dislodged and had to be reapplied when used with a seated manikin.
Conclusions: The NCCD can deliver chest compressions at target rate and depth to both supine and seated manikins with efficacy equivalent to manual CPR and the LUCAS 3. It can become dislodged when applied to a seated manikin; its design has now been altered to prevent this. New users can be trained in use of the NCCD quickly, but practise is required to ensure effective use.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Full article available here.
Diving Hyperb Med. 2023 September 30;53(3):189−202. doi: 10.28920/dhm53.3.189-202. PMID: 37718292. PMCID: PMC10597602.
Decompression procedures for transfer under pressure (‘TUP’) diving
Jan Risberg1, Pieter-Jan van Ooij2, Olav Sande Eftedal3
1 NUI, Bergen, Norway
2 Diving Medical Center, Royal Netherlands Navy, Den Helder, the Netherlands
3 Equinor, Trondheim, Norway
Corresponding author: Dr Jan Risberg, NUI, Gravdalsveien 245, 5165 Laksevåg, Bergen, Norway
Keywords
Bell diving; Decompression sickness; Decompression tables; Diving tables; Occupational diving
Abstract
(Risberg J, van Ooij P-J, Eftedal O. Decompression procedures for transfer under pressure (‘TUP’) diving. Diving and Hyperbaric Medicine. 2023 September 30;53(3):189−202. doi: 10.28920/dhm53.3.189-202. PMID: 37718292. PMCID: PMC10597602.)
Background: There is an increasing interest in ‘transfer under pressure’ (TUP) decompression in commercial diving, bridging traditional surface-oriented diving and saturation diving. In TUP diving the diver is surfaced in a closed bell and transferred isobarically to a pressure chamber for final decompression to surface pressure.
Methods: Tables for air diving and air and oxygen decompression have been compared for total decompression time (TDT), oxygen breathing time as well as high and low gradient factors (GF high and low). These have been considered surrogate outcome measures of estimated decompression sickness probability (PDCS).
Results: Six decompression tables from DadCoDat (DCD, The Netherlands), Defence and Civil Institute of Environmental Medicine (DCIEM, Canada), Comex MT92 tables (France) and the United States Navy (USN) have been compared. In general, USN and DCD procedures advised longer TDT and oxygen breathing time and had a lower GF high compared to MT92 and DCIEM tables. GF low was significantly higher in USN procedures compared to DCD and one of the MT92 tables due to a shallower first stop in many USN profiles compared to the two others. Allowance and restrictions for repetitive diving varied extensively between the six procedures. While USN procedures have been risk-assessed by probabilistic models, no detailed documentation is available for any of the tables regarding validation in experimental and operational diving.
Conclusions: Absence of experimental testing of the candidate tables precludes firm conclusions regarding differences in PDCS. All candidate tables are recognised internationally as well as within their national jurisdictions, and final decisions on procedure preference may depend on factors other than estimated PDCS. USN and DCD procedures would be expected to have lower PDCS than MT92 and DCIEM procedures, but the magnitude of these differences is not known.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Full article available here.
Diving Hyperb Med. 2023 September 30;53(3):203−209. doi: 10.28920/dhm53.3.203-209. PMID: 37718293. PMCID: PMC10735713.
Hyperbaric oxygen treatment in children: experience in 329 patients
Figen Aydin1
1 Department of Hyperbaric Medicine, University of Health Sciences, Izmir Bozyaka Training and Research Hospital, Izmir, Turkey
Corresponding author: Dr Figen Aydin, Saim Çıkrıkçı Cad. No:59, 35110 Karabağlar/İzmir, Turkey
Keywords
Barotrauma; Carbon monoxide; Hearing loss sudden; Safety; Side effects
Abstract
(Aydin F. Hyperbaric oxygen treatment in children: experience in 329 patients. Diving and Hyperbaric Medicine. 2023 September 30;53(3):203−209. doi: 10.28920/dhm53.3.203-209. PMID: 37718293. PMCID: PMC10735713.)
Introduction: Paediatric patients, like adults, may undergo hyperbaric oxygen treatment (HBOT) in both life-threatening situations and chronic diseases. There are particular challenges associated with managing paediatric patients for HBOT. This paper documents the indications, results, complications, and difficulties that occur during HBOT for a large cohort of paediatric patients and compares them with adult data in the literature. Methods used to reduce these difficulties and complications in children are also discussed.
Methods: This was a 15-year retrospective review of paediatric patients treated with HBOT at two hyperbaric centres. Between January 2006 and June 2021, patients under the age of 18 who received at least one session of HBOT were included.
Results: Three hundred and twenty-nine paediatric patients underwent a total of 3,164 HBOT exposures. Two-hundred and fifty-four patients (77.2%) completed treatment as planned and 218 (66.5%) achieved treatment goals without complications. Two patients treated for carbon monoxide poisoning exhibited neurological sequelae. Amputation was performed in one patient with limb ischaemia. Middle ear barotrauma events occurred in five treatments. No central nervous system oxygen toxicity was recorded during the treatments.
Conclusions: This patient series indicates that HBOT can be safely performed in pediatric patients with low complication rates by taking appropriate precautions. The cooperation of hyperbaric medicine physicians and other physicians related to paediatric healthcare is important in order for more patients to benefit from this treatment. When managing intubated patients an anaesthesiologist may need to participate in the treatment in order to perform necessary interventions.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Diving Hyperb Med. 2023 September 30;53(3):210−217. doi: 10.28920/dhm53.3.210-217. PMID: 37718294. PMCID: PMC10751292.
Snorkelling and breath-hold diving fatalities in Australian waters, 2014 to 2018
John Lippmann1,2,3
1 Australasian Diving Safety Foundation, Canterbury, Victoria, Australia
2 Department of Public Health and Preventive Medicine, Monash University, Victoria, Australia
3 Royal Life Saving Society Australia, Sydney, Australia
Corresponding author: Dr John Lippmann, Australasian Diving Safety Foundation, PO Box 478, Canterbury, VIC 3126, Australia
Keywords
Diving deaths; Cardiovascular; Fatalities; Freediving; Immersion; Snorkelling; Spearfishing
Abstract
(Lippmann J. Snorkelling and breath-hold diving fatalities in Australian waters, 2014 to 2018. Diving and Hyperbaric Medicine. 2023 September 30;53(3):210−217. doi: 10.28920/dhm53.3.210-217. PMID: 37718294. PMCID: PMC10751292.)
Introduction: This study investigated snorkelling and breath-hold diving deaths in Australia from 2014–2018 and compared these to those from 2001–2013 to identify ongoing problems and assess the effectiveness of countermeasures.
Methods: Media reports and the National Coronial Information System were searched to identify snorkelling/breath-hold diving deaths for 2014−2018, inclusive. Data were extracted from witness and police reports, medical histories, and autopsies. An Excel® database was created and a chain of events analysis conducted. Comparisons were made with the earlier report.
Results: Ninety-one fatalities (78 males, 13 females, median age 48 years [range 16−80]) were identified with one third likely doing some breath-hold diving. Fifty-two of 77 with known body mass index were overweight or obese. Approximately two thirds were inexperienced snorkellers and 64 were alone. Fifty-one were tourists. Planning shortcomings, such as solo diving and diving in adverse conditions, as well as pre-existing health conditions and inexperience predisposed to many incidents. Primary drowning was the likely disabling condition in 39% of cases with drowning recorded as the cause of death (COD) in two thirds. Cardiac events were the likely disabling conditions in 31% although recorded as the COD in 21% of cases.
Conclusions: Increasing age, obesity and associated cardiac disease have become increasingly prevalent in snorkelling deaths and there is a need for improved health surveillance and risk management. Closer supervision of inexperienced snorkellers is indicated. Apnoeic hypoxia from extended breath-holding and poor supervision remain a problem. The increased risk of harvesting seafood in areas frequented by large marine predators needs to be appreciated and managed appropriately.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Diving Hyperb Med. 2023 September 30;53(3):218−223. doi: 10.28920/dhm53.3.218-223. PMID: 37718295. PMCID: PMC10735697.
Self-reported vitality and health status are higher in Dutch submariners than in the general population
Antoinette Houtkooper1, Thijs T Wingelaar1,2 , Edwin L Endert1, Pieter-Jan AM van Ooij1,3
1 Royal Netherlands Navy Diving and Submarine Medical Center, Den Helder, the Netherlands
2 Amsterdam UMC, location AMC, Department of Anaesthesiology, Amsterdam, the Netherlands
3 Amsterdam UMC, location AMC, Department of Pulmonology, Amsterdam, the Netherlands
Corresponding author: Dr Thijs Wingelaar, Royal Netherlands Navy Diving Medical Center, Rijkszee en Marinehaven, PO Box 10.000, 1780 CA, Den Helder, the Netherlands
Keywords
Long-term health surveillance; Naval medicine; Occupational health; Quality of life; Submarine medicine
Abstract
(Houtkooper A, Wingelaar TT, Endert EL, van Ooij PJAM. Self-reported vitality and health status are higher in Dutch submariners than in the general population. Diving and Hyperbaric Medicine. 2023 September 30;53(3):218−223. doi: 10.28920/dhm53.3.218-223. PMID: 37718295. PMCID: PMC10735697.)
Introduction: Living aboard submarines has a potential negative effect on health. Although studies have evaluated specific health hazards and short-term outcomes, long-term health effects have not been investigated in this population.
Methods: Veteran submariners were contacted through the veterans’ society and administered a World Health Organisation validated questionnaire (SF-36) assessing their physical, emotional, and social functioning. Scores were compared with those of the general (reference) population and scores in veteran submariners were differentiated by rank, time at sea and time in service. Statistical analyses were performed using the Wilcoxon signed rank and Kruskal-Wallis tests.
Results: Of the 1,025 submariners approached in December 2019, 742 (72.4%) completed and returned the questionnaire before July 2020. All 742 were men, of median age 68 (interquartile range [IQR] 59–76) years (range 34–99 years). Of these subjects, 10.3% were current smokers, 64.4% were former smokers and 23.7% had never smoked. Submariners scored significantly better (P < 0.001) than the general population on all eight domains of the SF-36. Except for ‘pain’ and ‘change in health status over the last year’, scores for all domains decreased with age. Scores were not significantly affected by smoking status, rank, service, and time at sea.
Conclusions: Dutch veteran submariners have better self-reported vitality and health status than the general Dutch population. Rank, service, and time at sea did not significantly affect scores of Dutch submariners.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Diving Hyperb Med. 2023 September 30;53(3):224−229. doi: 10.28920/dhm53.3.224-229. PMID: 37718296. PMCID: PMC10735708.
Outcomes of hyperbaric oxygen treatment for central and branch retinal artery occlusion at a major Australian referral hospital
Jeremy Williamson1, Anil Sharma1, Alexander Murray-Douglass1, Matthew Peters1, Lawrence Lee1, Robert Webb2, Kenneth Thistlethwaite2, Thomas P Moloney1,3
1 Department of Ophthalmology, Royal Brisbane and Women’s Hospital, Brisbane, Australia
2 Department of Hyperbaric Medicine, Royal Brisbane and Women’s Hospital, Brisbane, Australia
3 School of Medicine, University of Queensland, Brisbane, Australia
Corresponding author: Dr Thomas P Moloney, Department of Ophthalmology, Royal Brisbane and Women’s Hospital, Brisbane, Australia
Keywords
Blindness; Circulation; Ophthalmology; Retinal artery occlusion; Vision
Abstract
(Williamson J, Sharma A, Murray-Douglass A, Peters M, Lee L, Webb R, Thistlethwaite K, Moloney TP. Outcomes of hyperbaric oxygen treatment for central and branch retinal artery occlusion at a major Australian referral hospital. Diving and Hyperbaric Medicine. 2023 September 30;53(3):224−229. doi: 10.28920/dhm53.3.224-229. PMID: 37718296. PMCID: PMC10735708.)
Introduction: This study analysed the treatment outcomes of patients that received hyperbaric oxygen treatment (HBOT) for retinal artery occlusion (RAO) at the Royal Brisbane and Women’s Hospital in Brisbane, Australia between 2015 and 2021.
Methods: Retrospective study from patient records including 22 eyes from 22 patients that received HBOT for either central RAO (17 patients) or branch RAO (five patients). Patients received the Royal Brisbane and Women’s Hospital RAO protocol for their HBOT. Analysis included best corrected visual acuity pre- and post-treatment, subjective improvements, side effects and patient risk factors were also recorded.
Results: Improvement in best corrected visual acuity was LogMAR -0.2 for central RAO on average with 8/17 (47%) experiencing objective improvement, 5/17 (29%) experienced no change and 4/22 (24%) experienced a reduction in best corrected visual acuity. Subjective improvement (colour perception or visual fields) was reported in an additional 4/17 patients, resulting in 12/17 (71%) reporting improvement either in visual acuity or subjectively. There was no improvement in the best corrected visual acuity of any of the five patients suffering from branch RAO. Cardiovascular risk factors present in the cohort included hypertension, hypercholesterolaemia, previous cardiovascular events, cardiac disease and smoking. Limited side effects were experienced by this patient cohort with no recorded irreversible side effects.
Conclusions: Hyperbaric oxygen treatment appears a safe, beneficial treatment for central RAO. No benefit was demonstrated in branch RAO although numbers were small. Increased awareness of HBOT for RAO resulting in streamlined referrals and transfers and greater uptake of this intervention may further improve patient outcomes.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Diving Hyperb Med. 2023 September 30;53(3):230−236. doi: 10.28920/dhm53.3.230-236. PMID: 37718297. PMCID: PMC10735644.
Contemporary practices of blood glucose management in diabetic patients: a survey of hyperbaric medicine units in Australia and New Zealand
Brenda R Laupland1, Kevin Laupland2,3, Kenneth Thistlethwaite1, Robert Webb1,4
1 Hyperbaric Medicine Unit, Royal Brisbane and Women’s Hospital, Brisbane, Australia
2 Queensland University of Technology (QUT), Brisbane, Australia
3 Department of Intensive Care Services, Royal Brisbane and Women’s Hospital, Brisbane, Australia
4 Clinical Informatics, Digital Metro North, Metro North Health, Brisbane, Australia
Corresponding author: Dr Brenda Laupland, Hyperbaric Medicine Unit, Royal Brisbane and Women’s Hospital, Butterfield Street, Herston, Queensland, 4029 Australia
ORCiD ID: 0009-0005-4883-1932
Keywords
Blood sugar level; Diabetes; Hyperbaric oxygen treatment; Protocol; Questionnaire
Abstract
(Laupland BR, Laupland K, Thistlethwaite K, Webb R. Contemporary practices of blood glucose management in diabetic patients: a survey of hyperbaric medicine units in Australia and New Zealand. Diving and Hyperbaric Medicine. 2023 September 30;53(3):230−236. doi: 10.28920/dhm53.3.230-236. PMID: 37718297. PMCID: PMC10735644.)
Introduction: Blood glucose levels may be influenced by hyperbaric oxygen treatment (HBOT). Patients with diabetes mellitus commonly receive HBOT but there is a lack of standardised blood glucose management guidelines. We documented relevant contemporary practices applied for patients with diabetes treated in hyperbaric medicine units.
Methods: A survey was administered in 2022 to the directors of all 13 accredited hyperbaric units in Australia and New Zealand to identify policies and practices related to management of patients with diabetes receiving HBOT.
Results: Twelve of the 13 units routinely managed patients with diabetes. Three-quarters (9/12) used < 4 mmol·l-1 as their definition of hypoglycaemia, whereas the other three used < 5, < 3.6, and < 3 mmol·l-1. Units reported 26% (range 13–66%) of their patients have a diagnosis of diabetes of which 93% are type 2. Ten (83%) units reported specific written protocols for managing blood glucose. Protocols were more likely to be followed by nursing (73%) than medical staff (45%). Ten (83%) units routinely tested blood glucose levels on all patients with diabetes. Preferred pre-treatment values for treatments in both multiplace and monoplace chambers ranged from ≥ 4 to ≥ 8 mmol·l-1. Seven (58%) units reported continuation of routine testing throughout a treatment course with five (42%) units having criteria-based rules for discontinuing testing for stable patients over multiple treatments. Two-thirds of units were satisfied with their current policy.
Conclusions: This survey highlights the burden of diabetes on patients treated with HBOT and identifies considerable variability in practices which may benefit from further study to optimise management of these patients.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Diving Hyperb Med. 2023 September 30;53(3):237−242. doi: 10.28920/dhm53.3.237-242. PMID: 37718298. PMCID: PMC10735703.
A retrospective review of the utility of Chest X-rays in diving and submarine medical examinations
Willem AJ Meintjes1, LaDonna R Davids1,2, Charles H van Wijk1,2
1 Division of Health Systems and Public Health, Faculty of Medicine and Health Sciences, Stellenbosch University, Stellenbosch, South Africa
2 Institute for Maritime Medicine, Simon's Town, Cape Town, South Africa
Corresponding author: Dr Willem AJ Meintjes, Division of Health Systems and Public Health, Faculty of Medicine and Health Sciences, Stellenbosch University, South Africa
ORCiD ID: 0000-0002-4909-5421
Keywords
Fitness to dive; Health surveillance; Medicals – diving; Occupational health; Occupational diving; Radiological imaging; Respiratory
Abstract
(Meintjes WAJ, Davids LR, van Wijk CH. A retrospective review of the utility of Chest X-rays in diving and submarine medical examinations. Diving and Hyperbaric Medicine. 2023 September 30;53(3):237−242. doi: 10.28920/dhm53.3.237-242. PMID: 37718298. PMCID: PMC10735703.)
Introduction: Performance of routine chest X-rays (CXRs) in asymptomatic individuals to assess hyperbaric exposure risk is controversial. The radiation risk may overshadow the low yield in many settings. However, the yield may be higher in certain settings, such as tuberculosis-endemic countries. We evaluated the utility of routine CXR in diving and submarine medical examinations in South Africa.
Methods: Records of 2,777 CXRs during 3,568 fitness examinations of 894 divers and submariners spanning 31 years were reviewed to determine the incidence of CXR abnormality. Associated factors were evaluated using odds ratios and a binomial logistic regression model, with a Kaplan-Meier plot to describe the duration of service until first abnormal CXR.
Results: An abnormal CXR was reported in 1.1% per person year of service, yielding a cumulative incidence of 6.5% (58/894) of the study participants. Only four individuals had a clinical indication for the CXR in their medical history. A range of potential pathologies were seen, of which 15.5% were declared disqualifying and the rest (84.5%) were treated, or further investigation showed that the person could be declared fit.
Conclusions: In South Africa, a routine CXR has a role to play in detecting abnormalities that are incompatible with pressure exposures. The highest number of abnormalities were found during the initial examinations and in individuals with long service records. Only four individuals had a clinical indication for their CXR during the 31-year span of our study. Similar studies should be performed to make recommendations in other countries and settings.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Diving Hyperb Med. 2023 September 30;53(3):243−250. doi: 10.28920/dhm53.3.243-250. PMID: 37718299. PMCID: PMC10735645.
A retrospective review of divers treated for inner ear decompression sickness at Fiona Stanley Hospital hyperbaric medicine unit 2014–2020
Jeremy S Mason1, Peter Buzzacott2, Ian C Gawthrope1,3, Neil D Banham1
1 Department of Hyperbaric Medicine, Fiona Stanley Hospital, Murdoch, WA, Australia
2 Prehospital, Resuscitation and Emergency Care Research Unit, Curtin School of Nursing, Curtin University, WA, Australia
3 University of Notre Dame, Fremantle, WA, Australia
Corresponding author: Dr Jeremy Mason, Department of Hyperbaric Medicine, Fiona Stanley Hospital, 11 Robin Warren Drive, Murdoch, WA, 6150, Australia
Keywords
Diving medicine; Diving research; ENT; Hyperbaric oxygen; Persistent (patent) foramen ovale (PFO); Right-to-left shunt; Vertigo
Abstract
(Mason JS, Buzzacott P, Gawthrope IC, Banham ND. A retrospective review of divers treated for inner ear decompression sickness at Fiona Stanley Hospital hyperbaric medicine unit 2014–2020. Diving and Hyperbaric Medicine. 2023 September 30;53(3):243−250. doi: 10.28920/dhm53.3.243-250. PMID: 37718299. PMCID: PMC10735645. )
Introduction: Inner ear decompression sickness (IEDCS) is increasingly recognised in recreational diving, with the inner ear particularly vulnerable to decompression sickness in divers with a right-to-left shunt, such as is possible through a persistent (patent) foramen ovale (PFO). A review of patients treated for IEDCS at Fiona Stanley Hospital Hyperbaric Medicine Unit (FSH HMU) in Western Australia was performed to examine the epidemiology, risk factors for developing this condition, the treatment administered and the outcomes of this patient population.
Methods: A retrospective review of all divers treated for IEDCS from the opening of the FSH HMU on 17 November 2014 to 31 December 2020 was performed. Patients were included if presenting with vestibular or cochlear dysfunction within 24 hours of surfacing from a dive, and excluded if demonstrating features of inner ear barotrauma.
Results: There were a total of 23 IEDCS patients and 24 cases of IEDCS included for analysis, with 88% experiencing vestibular manifestations and 38% cochlear. Median dive time was 40 minutes and median maximum depth was 24.5 metres. The median time from surfacing to hyperbaric oxygen treatment (HBOT) was 22 hours. Vestibulocochlear symptoms fully resolved in 67% and complete symptom recovery was achieved in 58%. A PFO was found in 6 of 10 patients who subsequently underwent investigation with bubble contrast echocardiography upon follow-up.
Conclusions: IEDCS occurred predominantly after non-technical repetitive air dives and ongoing symptoms and signs were often observed after HBOT. Appropriate follow-up is required given the high prevalence of PFO in these patients.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Diving Hyperb Med. 2023 September 30;53(3):251−258. doi: 10.28920/dhm53.3.251-258. PMID: 37718300. PMCID: PMC10735712.
Selecting optimal air diving gradient factors for Belgian military divers: more conservative settings are not necessarily safer
Sven De Ridder1,2, Nathalie Pattyn1, Xavier Neyt1, Peter Germonpré2
1 VIPER Research Unit, Royal Military Academy, Brussels, Belgium
2 Centre for Hyperbaric Oxygen Therapy, Military Hospital, Brussels, Belgium
Corresponding author: Sven De Ridder, Centre for Hyperbaric Oxygen Therapy, Military Hospital, Brussels, Bruynstraat 1, 1120 Brussels, Belgium
Keywords
Computers-diving; Decompression; Decompression sickness; Decompression tables; Diving; Simulation; Models
Abstract
(De Ridder S, Pattyn N, Neyt X, Germonpré P. Selecting optimal air diving gradient factors for Belgian military divers: more conservative settings are not necessarily safer. Diving and Hyperbaric Medicine. 2023 September 30;53(3):251−258. doi: 10.28920/dhm53.3.251-258. PMID: 37718300. PMCID: PMC10735712.)
Introduction: In 2018, the Belgian Defence introduced a commercial off-the-shelf dive computer (Shearwater Perdix™) for use by its military divers. There were operational constraints when using its default gradient factors (GF). We aimed to provide guidelines for optimal GF selection.
Methods: The Defence and Civil Institute of Environmental Medicine (DCIEM) dive tables and the United States Navy (USN) air decompression tables are considered acceptably safe by the Belgian Navy Diving Unit. The decompression model used in the Shearwater Perdix (Bühlmann ZH-L16C algorithm with GF) was programmed in Python. Using a sequential search of the parameter space, the GF settings were optimised to produce decompression schedules as close as possible to those prescribed by the USN and DCIEM tables.
Results: All reference profiles are approached when GFLO is kept equal to 100 and only GFHI is reduced to a minimum of 75 to prolong shallower stop times. Using the Perdix default settings (GFLO = 30 and GFHI = 70) yields deeper initial stops, leading to increased supersaturation of the ‘slower’ tissues, which potentially leads to an increased DCS risk. However, Perdix software does not currently allow for the selection of our calculated optimal settings (by convention GFLO < GFHI). A sub-optimal solution would be a symmetrical GF setting between 75/75 and 95/95.
Conclusions: For non-repetitive air dives, the optimal GF setting is GFLO 100, with only the GFHI parameter lowered to increase safety. No evidence was found that using the default GF setting (30/70) would lead to a safer decompression for air dives as deep as 60 metres of seawater; rather the opposite. Belgian Navy divers have been advised against using the default GF settings of the Shearwater Perdix dive computer and instead adopt symmetrical GF settings which is currently the optimal achievable approach considering the software constraints.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Diving Hyperb Med. 2023 September 30;53(3):259−267. doi: 10.28920/dhm53.3.259-267. PMID: 37718301. PMCID: PMC10735636.
Diving with psychotropic medication: review of the literature and clinical considerations
Abraham L Querido1,2, Chiel F Ebbelaar3,4,5, Thijs T Wingelaar2,6
1 Praktijk Querido, Hilversum, the Netherlands
2 Dutch Society of Diving and Hyperbaric Medicine, Bilthoven, the Netherlands
3 PharmC, consultancy for clinical psychopharmacology, Utrecht, the Netherlands
4 Leiden University Medical Center, Department of Dermatology, Leiden, the Netherlands
5 University Medical Center Utrecht, Department of Pathology, Division of Laboratories, Pharmacy and Biomedical
Genetics, University Medical Center Utrecht, Utrecht, the Netherlands
6 Royal Netherlands Navy, Diving Medical Center, Den Helder, the Netherlands
Corresponding author: Dr Thijs T Wingelaar, Rijkszee en Marinehaven, 1780 CA Den Helder, the Netherlands
Keywords
Fitness-to-dive; Medications; Mental health; Pharmacology; Psychiatry; Scuba
Abstract
(Querido AL, Ebbelaar CF, Wingelaar TT. Diving with psychotropic medication: review of the literature and clinical considerations. Diving and Hyperbaric Medicine. 2023 September 30;53(3):259−267. doi: 10.28920/dhm53.3.259-267. PMID: 37718301. PMCID: PMC10735636.)
This review discusses the safety concerns associated with diving while using psychotropic medication and the limited literature available on the topic. Despite the risks, some divers continue to dive while taking these medications, and their reasons for doing so are unclear. The exact mechanisms of action of these drugs in hyperbaric environments are poorly understood. While current standards and advice for fitness-to-dive assessments are based on limited evidence and expert opinion, developing evidence-based strategies could improve patient care and optimise diving safety. This review appraises relevant literature in diving medicine and provides clinical perspectives for diving physicians conducting fitness-to-dive assessments on patients using psychotropic medication.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Review article
Diving Hyperb Med. 2023 September 30;53(3):268−280. doi: 10.28920/dhm53.3.268-280. PMID: 37718302. PMCID: PMC10597603.
A systematic review of electroencephalography in acute cerebral hypoxia: clinical and diving implications
Nicole YE Wong1,2, Hanna van Waart1, Jamie W Sleigh1,3, Simon J Mitchell1,2,4, Xavier CE Vrijdag1
1 Department of Anaesthesiology, University of Auckland, Auckland, New Zealand
2 Department of Anaesthesia, Auckland City Hospital, Auckland, New Zealand
3 Department of Anaesthesia, Waikato Hospital, Hamilton, New Zealand
4 Slark Hyperbaric Unit, North Shore Hospital, Auckland, New Zealand
Corresponding author: Dr Xavier CE Vrijdag, Department of Anaesthesiology, School of Medicine, University of Auckland, Private bag 92019, Auckland 1142, New Zealand
ORCiD: 0000-0001-5907-6083
Keywords
Diving research; Diving safety memos; Physiology; Neurology; Brain
Abstract
(Wong NYE, van Waart H, Sleigh JW, Mitchell SJ, Vrijdag XCE. A systematic review of electroencephalography in acute cerebral hypoxia: clinical and diving implications. Diving and Hyperbaric Medicine. 2023 September 30;53(3):268−280. doi: 10.28920/dhm53.3.268-280. PMID: 37718302. PMCID: PMC10597603.)
Introduction: Hypoxia can cause central nervous system dysfunction and injury. Hypoxia is a particular risk during rebreather diving. Given its subtle symptom profile and its catastrophic consequences there is a need for reliable hypoxia monitoring. Electroencephalography (EEG) is being investigated as a real time monitor for multiple diving problems related to inspired gas, including hypoxia.
Methods: A systematic literature search identified articles investigating the relationship between EEG changes and acute cerebral hypoxia in healthy adults. Quality of clinical evidence was assessed using the Newcastle-Ottawa scale.
Results: Eighty-one studies were included for analysis. Only one study investigated divers. Twelve studies described quantitative EEG spectral power differences. Moderate hypoxia tended to result in increased alpha activity. With severe hypoxia, alpha activity decreased whilst delta and theta activities increased. However, since studies that utilised cognitive testing during the hypoxic exposure more frequently reported opposite results it appears cognitive processing might mask hypoxic EEG changes. Other analysis techniques (evoked potentials and electrical equivalents of dipole signals), demonstrated sustained regulation of autonomic responses despite worsening hypoxia. Other studies utilised quantitative EEG analysis techniques, (Bispectral index [BISTM], approximate entropy and Lempel-Ziv complexity). No change was reported in BISTM value, whilst an increase in approximate entropy and Lempel-Ziv complexity occurred with worsening hypoxia.
Conclusions: Electroencephalographic frequency patterns change in response to acute cerebral hypoxia. There is paucity of literature on the relationship between quantitative EEG analysis techniques and cerebral hypoxia. Because of the conflicting results in EEG power frequency analysis, future research needs to quantitatively define a hypoxia-EEG response curve, and how it is altered by concurrent cognitive task loading.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Review article
Diving Hyperb Med. 2023 September 30;53(3):281−284. doi: 10.28920/dhm53.3.281-284. PMID: 37718303. PMCID: PMC10735667.
Investigation into the effect of hyperbaric hyperoxia on serum cardiac Troponin T levels as a biomarker of cardiac injury
Jack Marjot1, John Mackenzie1, Nigel Jepson2, Ewan Reeves1, Michael Bennett1
1 Department of Diving and Hyperbaric Medicine, Prince of Wales Hospital, Sydney
2 Department of Cardiology, Prince of Wales Hospital, Sydney
Corresponding author: Dr Jack Marjot, Department of Diving and Hyperbaric Medicine, Prince of Wales Hospital, Sydney, Australia
ORCiD ID: 0009-0002-0212-1343
Keywords
Biomarkers; Cardiovascular; Health; Heart; Hyperbaric oxygen treatment
Abstract
(Marjot J, Mackenzie J, Jepson N, Reeves E, Bennett M. Investigation into the effect of hyperbaric hyperoxia on serum cardiac Troponin T levels as a biomarker of cardiac injury. Diving and Hyperbaric Medicine. 2023 September 30;53(3):281−284. doi: 10.28920/dhm53.3.281-284. PMID: 37718303. PMCID: PMC10735667.)
Introduction: There is clinical equipoise as to whether hyperoxia is injurious to the myocardium, both in the setting of acute ischaemic insults and on the stable myocardium. This study examined the effect of extreme hyperoxia – in the form of hyperbaric oxygen treatment – on the myocardium through measurement of high-sensitivity cardiac troponin.
Methods: Forty-eight individuals were enrolled to undergo a series of 30 exposures to hyperbaric oxygen for treatment of non-cardiac pathologies. High-sensitivity troponin T was measured before and after each session.
Results: There was no clinically significant difference in troponin measurements following acute or recurrent sequential exposures to extreme hyperoxia, despite the studied patient population having a high rate of previous ischaemic heart disease or cardiovascular risk factors.
Conclusions: This study demonstrates that profound hyperoxaemia does not induce any measurable cardiac injury at a biochemical level. Neither is there a reduction in cardiac troponin to suggest a cardioprotective effect of hyperbaric hyperoxia. This provides some reassurance as to the cardiac safety of the routine use of hyperbaric oxygen treatment in management of non-cardiac pathology.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Short communication
Diving Hyperb Med. 2023 September 30;53(3):285−289. doi: 10.28920/dhm53.3.285-289. PMID: 37718304. PMCID: PMC10735701.
Atypical distally distributed cutis marmorata decompression sickness associated with unconventional use of thermal protection in a diver with persistent foramen ovale
Petra Magri Gatt1, Emily Diacono2, Lyubisa Matity3, Kurt Magri4
1 Department of Medicine, Mater Dei Hospital, Msida, Malta
2 University of Malta, Msida, Malta
3 Hyperbaric and Tissue Viability Unit, Gozo General Hospital, Victoria, Gozo
4 Baromedicine Department, Hyperbaric Unit, Mater Dei Hospital, Msida, Malta
Corresponding author: Ms Emily Diacono, University of Malta, Msida, Malta
Keywords
Decompression illness; Pathophysiology; Right-to-left shunt; Wetsuit
Abstract
(Magri Gatt P, Diacono E, Matity L, Magri K. Atypical distally-distributed cutis marmorata decompression sickness associated with unconventional use of thermal protection in a diver with persistent foramen ovale. Diving and Hyperbaric Medicine. 2023 September 30;53(3):285−289. doi: 10.28920/dhm53.3.285-289. PMID: 37718304. PMCID: PMC10735701.)
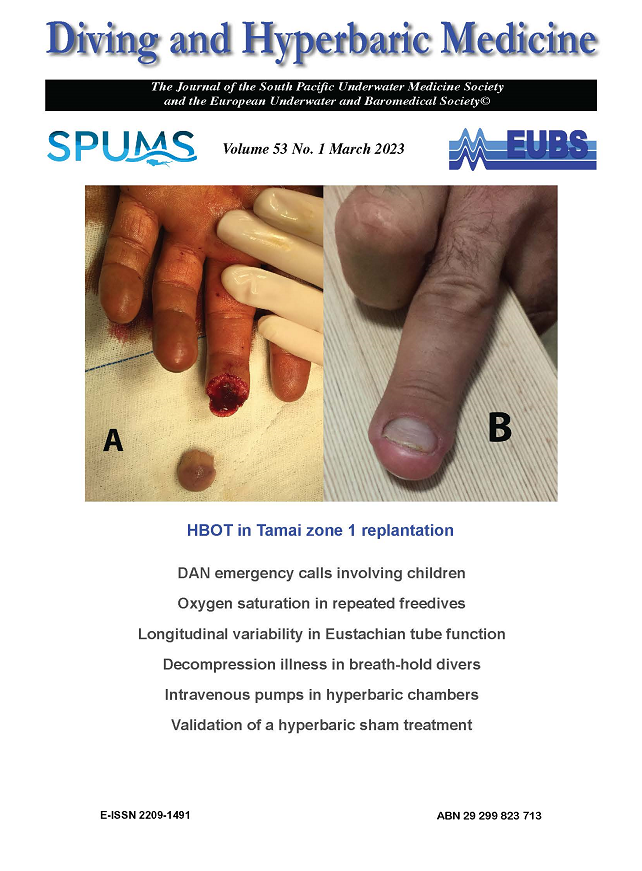
Cutis marmorata is a mottled, marbling, livedoid rash caused by vascular inflammation and congestion in cutaneous decompression sickness. It may occur during or after ascent due to the formation of bubbles from dissolved nitrogen accumulated throughout the dive. It is strongly associated with the presence of right to left shunts, particularly persistent (patent) foramen ovale (PFO). We report a case of cutis marmorata decompression sickness of an unusual pattern associated with unconventional use of thermal protection (a ‘shorty’ wetsuit worn over full suit) by a diver with a PFO. The patient also had neurological manifestations of decompression sickness. The distal lower limb pattern of involvement favours the hypothesis that cutis marmorata in humans is likely to be due to bubbles in the skin itself and/or adjacent tissues rather than cerebrally mediated.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Case report
Diving Hyperb Med. 2023 September 30;53(3):290-291. doi: 10.2890/dhm53.3.290-291. PMID: 37718305. PMCID: PMC10735711.
Commentary on Plogmark, et al. Agreement between ultrasonic bubble grades using a handheld self-positioning Doppler product and 2D cardiac ultrasound
Asya Metelkina1, Axel Barbaud1
1 Azoth Systems, Ollioules, France
Corresponding author: Axel Barbaud, Azoth Systems, 93 Forum de la Mediterranée, 83190, Ollioules, France
Keywords
Decompression sickness; Doppler; Risk Factors; Risk Management; Scuba diving; Venous gas emboli
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Letter to the Editor
Diving Hyperb Med. 2023 September 30;53(3):291. doi: 10.2890/dhm53.3.291. PMID: 37718306. PMCID: PMC10735709.
Response to Metelkina and Barbaud
Oscar Plogmark1,2, Carl Hjelte1,2,3, Magnus Ekström1, Oskar Frånberg2,4
1 Lund University, Faculty of Medicine, Department of Clinical Sciences Lund, Respiratory Medicine and Allergology, Lund, Sweden
2 Swedish Armed Forces Diving and Naval Medicine Center, Swedish Armed Forces, Karlskrona, Sweden
3 Sahlgrenska University Hospital, Anesthesia and Intensive Care, Gothenburg, Sweden
4 Blekinge Institute of Technology, Department of Mathematics and Natural Science, Karlskrona, Sweden
Corresponding author: Oscar Plogmark, Sten Bergmans väg 21, 121 46 Johanneshov, Sweden
Keywords
Decompression sickness; Doppler; Risk Factors; Risk Management; Scuba diving; Venous gas emboli
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Letter to the Editor
Diving Hyperb Med. 2023 September 30;53(3):292. doi: 10.2890/dhm53.3.292. PMID: 37718307. PMCID: PMC10735702.
Carbon monoxide poisoning: lest we forget
Bruce Mathew1, Gerard Laden1
1 Clinical Hyperbaric Facility, Hull and East Riding Hospital, Hull, UK
Corresponding author: Bruce Mathew, Clinical Hyperbaric Facility, Hull and East Riding Hospital, Hull, UK
ORCiD ID: 0009-0008-0820-8291
Keywords
Diving; Fatality; Gas supply; Scuba; Surface supply; Toxicity
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Letter to the Editor
- Super User
- Category: Information
- 2382
Click to download each article. This will download a PDF that is password protected from any changes, these individual article PDFs are not for public distribution and for society members personal use.
Copyright: These articles are the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
- Super User
- Category: Information
- 9801
2023 December;53(4)
Diving Hyperb Med. 2023 December 20;53(4):299−305. doi: 10.28920/dhm53.4.299-305. PMID: 38091588. PMCID: PMC10944666.
Risk assessment of SWEN21 a suggested new dive table for the Swedish armed forces: bubble grades by ultrasonography
Carl Hjelte1,2,3, Oskar Plogmark1,2, Mårten Silvanius2,4, Magnus Ekström1, Oskar Frånberg1,4
1 Lund University, Faculty of Medicine, Department of Clinical Sciences Lund, Respiratory Medicine and Allergology,
Lund, Sweden
2 Swedish Armed Forces Diving and Naval Medicine Center, Swedish Armed Forces, Karlskrona, Sweden
3 Sahlgrenska University Hospital, Anesthesia and Intensive Care, Gothenburg, Sweden
4 Blekinge Institute of Technology, Department of Mathematics and Natural Science, Karlskrona, Sweden
Corresponding author: Dr Carl Hjelte, Kungsladugårdsgatan 113B. 414 76, Gothenburg, Sweden
ORCiD: 0009-0009-5522-8735
carl_hjelte@hotmail
Keywords
Decompression; Decompression illness; Decompression tables; Diving; Echocardiography; Risk; Venous gas emboli
Abstract
(Hjelte C, Plogmark O, Silvanius M, Ekström M, Frånberg O. Risk assessment of SWEN21 a suggested new dive table for the Swedish armed forces: bubble grades by ultrasonography. Diving and Hyperbaric Medicine. 2023 December 20;53(4):299−305. doi: 10.28920/dhm53.4.299-305. PMID: 38091588. PMCID: PMC10944666.)
Introduction: To develop the diving capacity in the Swedish armed forces the current air decompression tables are under revision. A new decompression table named SWEN21 has been created to have a projected risk level of 1% for decompression sickness (DCS) at the no stop limits. The aim of this study was to evaluate the safety of SWEN21 through the measurement of venous gas emboli (VGE) in a dive series.
Methods: A total 154 dives were conducted by 47 divers in a hyperbaric wet chamber. As a proxy for DCS risk serial VGE measurements by echocardiography were conducted and graded according to the Eftedal-Brubakk scale. Measurements were done every 15 minutes for approximately 2 hours after each dive. Peak VGE grades for the different dive profiles were used in a Bayesian approach correlating VGE grade and risk of DCS. Symptoms of DCS were continually monitored.
Results: The median (interquartile range) peak VGE grade after limb flexion for a majority of the time-depth combinations, and of SWEN21 as a whole, was 3 (3–4) with the exception of two decompression profiles which resulted in a grade of 3.5 (3–4) and 4 (4–4) respectively. The estimated risk of DCS in the Bayesian model varied between 4.7–11.1%. Three dives (2%) resulted in DCS. All symptoms resolved with hyperbaric oxygen treatment.
Conclusions: This evaluation of the SWEN21 decompression table, using bubble formation measured with echocardiography, suggests that the risk of DCS may be higher than the projected 1%.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Diving Hyperb Med. 2023 December 20;53(4):306−312. doi: 10.28920/dhm53.4.306-312. PMID: 38091589. PMCID: PMC10944662.
Rapture of the deep: gas narcosis may impair decision-making in scuba divers
Pauliina A Ahti1, Jan Wikgren1
1 Centre for Interdisciplinary Brain Research, Department of Psychology, University of Jyväskylä, Finland
Corresponding author: Dr Pauliina A Ahti, Centre for Interdisciplinary Brain Research, Department of Psychology,
University of Jyväskylä, Finland
ORCiD: 000-002-6216-9616
Keywords
Cold; Deep diving; Gases; Nitrogen narcosis; Personality; Psychology; Scientific diving
Abstract
(Ahti PA, Wikgren J. Rapture of the deep: gas narcosis may impair decision-making in scuba divers. Diving and Hyperbaric Medicine. 2023 December 20;53(4):306−312. doi: 10.28920/dhm53.4.306-312. PMID: 38091589. PMCID: PMC10944662.)
Introduction: While gas narcosis is familiar to most divers conducting deep (> 30 metres) dives, its effects are often considered minuscule or subtle at 30 metres. However, previous studies have shown that narcosis may affect divers at depths usually considered safe from its influence, but little knowledge exists on the effects of gas narcosis on higher cognitive functions such as decision-making in relatively shallow water at 30 metres. Impaired decision-making could be a significant safety issue for a multitasking diver.
Methods: We conducted a study exploring the effects of gas narcosis on decision-making in divers breathing compressed air underwater. The divers (n = 22) were evenly divided into 5-metre and 30-metre groups. In the water, we used underwater tablets equipped with the Iowa Gambling Task (IGT), a well-known psychological task used to evaluate impairment in decision-making.
Results: The divers at 30 metres achieved a lower score (mean 1,584.5, standard deviation 436.7) in the IGT than the divers at 5 metres (mean 2,062.5, standard deviation 584.1). Age, body mass index, gender, or the number of previous dives did not affect performance in the IGT.
Conclusions: Our results suggest that gas narcosis may affect decision-making in scuba divers at 30 metres depth. This supports previous studies showing that gas narcosis is present at relatively shallow depths and shows that it may affect higher cognitive functions.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Diving Hyperb Med. 2023 December 20;53(4):313−320. doi: 10.28920/dhm53.4.313-320. PMID: 38091590. PMCID: PMC10735670.
Full-face snorkel masks increase the incidence of hypoxaemia and hypercapnia during simulated snorkelling compared to conventional snorkels
Janneke Grundemann1, Xavier CE Vrijdag1, Nicole YE Wong2, Nicholas Gant3, Simon J Mitchell1,2,4, Hanna van Waart1
1 Department of Anaesthesiology, University of Auckland, Auckland, New Zealand
2 Department of Anaesthesia, Auckland City Hospital, Auckland, New Zealand
3 Department of Exercise Sciences, University of Auckland, New Zealand
4 Slark Hyperbaric Unit, North Shore Hospital, Auckland, New Zealand
Corresponding author: Dr Hanna van Waart, Department of Anaesthesiology, School of Medicine, University of Auckland,
Private Bag 92019, Auckland 1142, New Zealand
ORCiD: 0000-0002-6931-0168
Keywords
Diving research; Equipment; Hypercapnia; Hypoxia; Safety
Abstract
(Grundemann J, Vrijdag XCE, Wong NYE, Gant N, Mitchell SJ, van Waart H. Full-face snorkel masks increase the incidence of hypoxaemia and hypercapnia during simulated snorkelling compared to conventional snorkels. Diving and Hyperbaric Medicine. 2023 December 20;53(4):313−320. doi: 10.28920/dhm53.4.313-320. PMID: 38091590. PMCID: PMC10735670.)
Introduction: Air flow in full-face snorkel masks (FFSMs) should be unidirectional to prevent rebreathing of exhaled air. This study evaluated rebreathing and its consequences when using full-face snorkel masks compared to a conventional snorkel.
Methods: In a dry environment 20 participants wore three types of snorkel equipment in random order: Subea Easybreath FFSM; QingSong 180-degree panoramic FFSM; and a Beuchat Spy conventional snorkel (with nose clip), in three conditions: rest in a chair; light; and moderate intensity exercise on a cycle ergometer. Peripheral oxygen saturation, partial pressure of carbon dioxide (PCO2) and oxygen (PO2) in the end tidal gas and FFSM eye-pockets, respiratory rate, minute ventilation, were measured continuously. Experiments were discontinued if oxygen saturation dropped below 85%, or if end-tidal CO2 exceeded 7.0 kPa.
Results: Experimental runs with the FFSMs had to be discontinued more often after exceeding 7.0 kPa end-tidal CO2 compared to a conventional snorkel e.g., 18/40 (45%) versus 4/20 (20%) during light intensity exercise, and 9/22 (41%) versus 3/16 (19%) during moderate intensity exercise. Thirteen participants exhibited peripheral oxygen saturations below 95% (nine using FFSMs and four using the conventional snorkel) and five fell below 90% (four using FFSMs and one using the conventional snorkel). The PCO2 and PO2 in the eye-pockets of the FFSMs fluctuated and were significantly higher and
lower respectively than in inspired gas, which indicated rebreathing in all FFSM wearers.
Conclusions: Use of FFSMs may result in rebreathing due to non-unidirectional flow, leading to hypercapnia and hypoxaemia.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Full article available here.
Diving Hyperb Med. 2023 December 20;53(4):321−326. doi: 10.28920/dhm53.4.321-326. PMID: 38091591. PMCID: PMC10944667.
Measuring whole body inert gas wash-out
Oscar Plogmark1,2, Mårten Silvanius3, Max Olsson1, Carl Hjelte1,2, Magnus Ekström1, Oskar Frånberg1,3
1 Lund University, Faculty of Medicine, Department of Clinical Sciences Lund, Respiratory Medicine and Allergology, Lund, Sweden
2 Swedish Armed Forces Diving and Naval Medicine Center, Swedish Armed Forces, Karlskrona, Sweden
3 Blekinge Institute of Technology, Department of Mathematics and Natural Science, Karlskrona, Sweden
Corresponding author: Oscar Plogmark, Sölvegatan 19, 221 85 Lund, Sweden
ORCiD: 0009-0008-3230-8807
Keywords
Decompression sickness; Diving research; Gas kinetics; Nitrogen; Physiology; Pressure
Abstract
(Plogmark O, Silvanius M, Olsson M, Hjelte C, Ekström M, Frånberg O. Measuring whole body inert gas wash-out. Diving and Hyperbaric Medicine. 2023 December 20;53(4):321−326. doi: 10.28920/dhm53.4.321-326. PMID: 38091591. PMCID: PMC10944667.)
Introduction: Quantifying inert gas wash-out is crucial to understanding the pathophysiology of decompression sickness. In this study, we developed a portable closed-circuit device for measuring inert gas wash-out and validated its precision and accuracy both with and without human subjects.
Methods: We developed an exhalate monitor with sensors for volume, temperature, water vapor and oxygen. Inert gas volume was extrapolated from these inputs using the ideal gas law. The device’s ability to detect volume differences while connected to a breathing machine was analysed by injecting a given gas volume eight times. One hundred and seventy-two coupled before-and-after measurements were then compared with a paired t-test. Drift in measured inert gas volume during unlabored breathing was evaluated in three subjects at rest using multilevel linear regression. A quasi-experimental crossover study with the same subjects was conducted to evaluate the device’s ability to detect inert gas changes in relation to diving interventions and simulate power.
Results: The difference between the injected volume (1,996 ml) and the device’s measured volume (1,986 ml) was -10 ml. The 95% confidence interval (CI) for the measured volume was 1,969 to 2,003 ml. Mean drift during a 43 min period of unlaboured breathing was -19 ml, (95% CI, -37 to -1). Our power simulation, based on a cross-over study design, determined a sample size of two subjects to detect a true mean difference of total inert gas wash-out volume of 100 ml.
Conclusions: We present a portable device with acceptable precision and accuracy to measure inert gas wash-out differences that may be physiologically relevant in the pathophysiology of decompression sickness.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Diving Hyperb Med. 2023 December 20;53(4):327−332. doi: 10.28920/dhm53.4.327-332. PMID: 38091592. PMCID: PMC10735710.
Comparing the EMMA capnograph with sidestream capnography and arterial carbon dioxide pressure at 284 kPa
Xavier CE Vrijdag1, Hanna van Waart1, Chris Sames2, Jamie W Sleigh1,3, Simon J Mitchell1,2,4
1 Department of Anaesthesiology, University of Auckland, Auckland, New Zealand
2 Slark Hyperbaric Unit, Waitemata District Health Board, Auckland, New Zealand
3 Department of Anaesthesia, Waikato Hospital, Hamilton, New Zealand
4 Department of Anaesthesia, Auckland City Hospital, Auckland, New Zealand
Corresponding author: Xavier Vrijdag, Department of Anaesthesiology, School of Medicine, University of Auckland, Private bag 92019, Auckland 1142, New Zealand
Keywords
Capnography; Hyperbaric chamber; Intensive care; Patient monitoring
Abstract
(Vrijdag XCE, van Waart H, Sames C, Sleigh JW, Mitchell SJ. Comparing the EMMA capnograph with sidestream capnography and arterial carbon dioxide pressure at 284 kPa. Diving and Hyperbaric Medicine. 2023 December 20;53(4):327−332. doi: 10.28920/dhm53.4.327-332. PMID: 38091592. PMCID: PMC10735710.)
Introduction: Capnography aids assessment of the adequacy of mechanical patient ventilation. Physical and physiological changes in hyperbaric environments create ventilation challenges which make end-tidal carbon dioxide (ETCO2) measurement particularly important. However, obtaining accurate capnography in hyperbaric environments is widely considered difficult. This study investigated the EMMA capnograph for hyperbaric use.
Methods: We compared the EMMA capnograph to sidestream capnography and the gold standard arterial carbon dioxide blood gas analysis in a hyperbaric chamber. In 12 resting subjects breathing air at 284 kPa, we recorded ETCO2 readings simultaneously derived from the EMMA and sidestream capnographs during two series of five breaths (total 24 measurements). An arterial blood gas sample was also taken simultaneously in five participants.
Results: Across all measurements there was a difference of about 0.1 kPa between the EMMA and sidestream capnographs indicating a very slight over-estimation of ETCO2 by the EMMA capnograph, but fundamentally good agreement between the two end-tidal measurement methods. Compared to arterial blood gas pressure the non-significant difference was about 0.3 and 0.4 kPa for the EMMA and sidestream capnographs respectively.
Conclusions: In this study, the EMMA capnograph performed equally to the sidestream capnograph when compared directly, and both capnography measures gave clinically acceptable estimates of arterial PCO2.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Full article available here.
Diving Hyperb Med. 2023 December 20;53(4):333−339. doi: 10.28920/dhm53.4.333-339. PMID: 38091593. PMCID: PMC10944664.
Within-diver variability in venous gas emboli (VGE) following repeated dives
David J Doolette1,2, F Gregory Murphy1
1 Navy Experimental Diving Unit, Panama City, Florida, USA
2 Department of Anaesthesiology, University of Auckland, New Zealand
Corresponding author: Associate Professor David J Doolette, Navy Experimental Diving Unit, Panama City, Florida, USA
ORCiD: 0000-0001-9027-3536
Keywords
Bubbles; Decompression sickness; Diving; Echocardiography; Risk
Abstract
(Doolette DJ, Murphy FG. Within-diver variability in venous gas emboli (VGE) following repeated dives. Diving and Hyperbaric Medicine. 2023 December 20;53(4):333−339. doi: 10.28920/dhm53.4.333-339. PMID: 38091593. PMCID: PMC10944664.)
Introduction: Venous gas emboli (VGE) are widely used as a surrogate endpoint instead of decompression sickness (DCS) in studies of decompression procedures. Peak post-dive VGE grades vary widely following repeated identical dives but little is known about how much of the variability in VGE grades is proportioned between-diver and within-diver.
Methods: A retrospective analysis of 834 man-dives on six dive profiles with post-dive VGE measurements were conducted under controlled laboratory conditions. Among these data, 151 divers did repeated dives on the same profile on two to nine occasions separated by at least one week (total of 693 man-dives). Data were analysed for between- and within-diver variability in peak post-dive VGE grades using mixed-effect models with diver as the random variable and associated intraclass correlation coefficients.
Results: Most divers produced a wide range of VGE grades after repeated dives on the same profile. The intraclass correlation coefficient (repeatability) was 0.33 indicating that 33% of the variability in VGE grades is between-diver variability; correspondingly, 67% of variability in VGE grades is within-diver variability. DCS cases were associated with an individual diver’s highest VGE grades and not with their lower VGE grades.
Conclusions: These data demonstrate large within-diver variability in VGE grades following repeated dives on the same dive profile and suggest there is substantial within-diver variability in susceptibility to DCS. Post-dive VGE grades are not useful for evaluating decompression practice for individual divers.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Diving Hyperb Med. 2023 December 20;53(4):340−344. doi: 10.28920/dhm53.4.340-344. PMID: 38091594. PMCID: PMC10944665.
Pulmonary oxygen toxicity breath markers after heliox diving to 81 metres
Feiko JM de Jong1,2, Paul Brinkman3, Thijs T Wingelaar1,2, Pieter-Jan AM van Ooij1,3, Robert A van Hulst2
1 Royal Netherlands Navy Diving and Submarine Medical Centre, 1780 CA, Den Helder, The Netherlands
2 Department of Anesthesiology, Amsterdam University Medical Center, location AMC, 1100 DD, Amsterdam, The Netherlands
3 Department of Pulmonology, Amsterdam University Medical Center, location AMC, 1100 DD, Amsterdam, The Netherlands
Corresponding author: Feiko JM de Jong, Royal Netherlands Navy Diving and Submarine Medical Centre, Rijkszee-en, Marinehaven, Postbus 10.000, 1780 CA, Den Helder, The Netherlands
ORCiD: 0009-0008-9804-8307
Keywords
Diving research; Helium; Military diving; Unit pulmonary toxic dose; Volatile organic compounds
Abstract
(de Jong FJM, Brinkman P, Wingelaar TT, van Ooij PJAM, van Hulst RA. Pulmonary oxygen toxicity breath markers after heliox diving to 81 metres. Diving and Hyperbaric Medicine. 2023 December 20;53(4):340−344. doi: 10.28920/dhm53.4.340-344. PMID: 38091594. PMCID: PMC10944665.)
Pulmonary oxygen toxicity (POT), an adverse reaction to an elevated partial pressure of oxygen in the lungs, can develop as a result of prolonged hyperbaric hyperoxic conditions. Initially starting with tracheal discomfort, it results in pulmonary symptoms and ultimately lung fibrosis. Previous studies identified several volatile organic compounds (VOCs) in exhaled breath indicative of POT after various wet and dry hyperbaric hypoxic exposures, predominantly in laboratory settings. This study examined VOCs after exposures to 81 metres of seawater by three navy divers during operational heliox diving. Univariate testing did not yield significant results. However, targeted multivariate analysis of POT-associated VOCs identified significant (P = 0.004) changes of dodecane, tetradecane, octane, methylcyclohexane, and butyl acetate during the 4 h post-dive sampling period. No airway symptoms or discomfort were reported. This study demonstrates that breath sampling can be performed in the field, and VOCs indicative of oxygen toxicity are exhaled without clinical symptoms of POT, strengthening the belief that POT develops on a subclinical-to-symptomatic spectrum. However, this study was performed during an actual diving operation and therefore various confounders were introduced, which were excluded in previous laboratory studies. Future studies could focus on optimising sampling protocols for field use to ensure uniformity and reproducibility, and on establishing dose-response relationships.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Short communication
Diving Hyperb Med. 2023 December 20;53(4):345−350. doi: 10.28920/dhm53.4.345-350. PMID: 38091595. PMCID: PMC10944668.
Cerebral arterial gas embolism (CAGE) during open water scuba certification training whilst practising a controlled emergency swimming ascent
Neil Banham1, Elisabete da Silva1, John Lippmann2
1 Department of Hyperbaric Medicine, Fiona Stanley Hospital, Murdoch, Australia
2 Australasian Diving Safety Foundation, Melbourne, Australia
Corresponding author: Dr Neil Banham, Department of Hyperbaric Medicine, Fiona Stanley Hospital, 11 Warren Drive,
Murdoch WA 6150, Australia
Keywords
Case reports; CESA; Diving accidents; Emergency ascent; Pneumomediastinum; Pneumothorax; Pulmonary barotrauma
Abstract
(Banham N, da Silva E, Lippmann J. Cerebral arterial gas embolism (CAGE) during open water scuba certification training whilst practising a controlled emergency swimming ascent. Diving and Hyperbaric Medicine. 2023 December 20;53(4):345−350. doi: 10.28920/dhm53.4.345-350. PMID: 38091595. PMCID: PMC10944668.)
We report the case of a 23-year-old male novice diver who sustained cerebral arterial gas embolism (CAGE) during his open water certification training whilst practising a free ascent as part of the course. He developed immediate but transient neurological symptoms that had resolved on arrival to hospital. Radiological imaging of his chest showed small bilateral pneumothoraces, pneumopericardium and pneumomediastinum. In view of this he was treated with high flow normobaric oxygen rather than recompression, because of the risk of development of tension pneumothorax upon chamber decompression. There was no relapse of his neurological symptoms with this regimen. The utility and safety of free ascent training for recreational divers is discussed, as is whether a pneumothorax should be vented prior to recompression, as well as return to diving following pulmonary barotrauma.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Case report
Diving Hyperb Med. 2023 December 20;53(4):351−355. doi: 10.28920/dhm53.4.351-355. PMID: 38091596. PMCID: PMC10944663.
Hyperbaric oxygen treatment in delayed post-hypoxic encephalopathy following inhalation of liquefied petroleum gas: a case report
Kubra Canarslan Demir1, Burak Turgut1, Kubra Ozgok Kangal1, Taylan Zaman1, Kemal Şimşek1
1 Underwater and Hyperbaric Medicine, University of Health Sciences, Gulhane Training and Research Hospital, Ankara, Turkey
Corresponding author: Dr Kübra Canarslan Demir, SBÜ-Gülhane Eğitim ve Araştırma Hastanesi, Sualtı Hekimliği ve Hiperbarik Tıp Kliniği, Etlik/Ankara, Turkey
ORCiD: 0000-0001-6911-2375
Keywords
Brain; Dementia; Hyperbaric medicine; Neurology; Toxicity
Abstract
(Canarslan Demir K, Turgut B, Ozgok Kangal K, Zaman T, Şimşek K. Hyperbaric oxygen treatment in delayed posthypoxic encephalopathy following inhalation of liquefied petroleum gas: a case report. Diving and Hyperbaric Medicine. 2023 December 20;53(4):351−355. doi: 10.28920/dhm53.4.351-355. PMID: 38091596. PMCID: PMC10944663.)
Delayed post-hypoxic encephalopathy can occur after an episode of anoxia or hypoxia. Symptoms include apathy, confusion, and neurological deficits. We describe a 47-year-old male patient who inhaled gas from a kitchen stove liquid petroleum gas cylinder. He was diagnosed with hypoxic ischaemic encephalopathy 12 hours after his emergency department admission. He received six sessions of hyperbaric oxygen treatment (HBOT) and was discharged in a healthy state after six days. Fifteen days later, he experienced weakness, loss of appetite, forgetfulness, depression, balance problems, and inability to perform self-care. One week later, he developed urinary and fecal incontinence and was diagnosed with post-hypoxic encephalopathy. After 45 days from the onset of symptoms, he was referred to the Underwater and Hyperbaric Medicine Department for HBOT. The patient exhibited poor self-care and slow speech rate, as well as ataxic gait and dysdiadochokinesia. Hyperbaric oxygen was administered for twenty-four sessions, which significantly improved the patient’s neurological status with only hypoesthesia in the left hand remaining at the end of treatment. Hyperbaric oxygen has been reported as successful in treating some cases of delayed neurological sequelae following CO intoxication. It is possible that HBO therapy may also
be effective in delayed post-hypoxic encephalopathy from other causes. This may be achieved through mechanisms such as transfer of functional mitochondria to the injury site, remyelination of damaged neurons, angiogenesis and neurogenesis, production of anti-inflammatory cytokines, and balancing of inflammatory and anti-inflammatory cytokines.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Case report
Diving Hyperb Med. 2023 December 20;53(4):356−359. doi: 10.28920/dhm53.4.356-359. PMID: 38091597. PMCID: PMC10944661.
Hypoxic loss of consciousness in air diving: two cases of mixtures made hypoxic by oxidation of the scuba diving cylinder
Arnaud Druelle1, Lucille Daubresse1, Jean U Mullot2, Hélène Streit3, Pierre Louge4
1 Department of Hyperbaric Medicine, Military Teaching Hospital, Sainte-Anne, Toulon, France
2 Navy Laboratory for Analysis Surveillance and Expertise, 83000 Toulon, France
3 Medical Center of ATRIA, 90 000 BELFORT, France
4 Acute Medicine Department, Hyperbaric Medicine Unit, Geneva University Hospitals, rue Gabrielle-Perret-Gentil 4, 1205 Geneva, Switzerland
Corresponding author: Dr Arnaud Druelle, Department of Hyperbaric Medicine, Military Teaching Hospital, HIA Ste Anne, 2 boulevard Ste Anne, BP 600, 83800 Toulon CEDEX, France
Keywords
Case reports; Corrosion; Diving tank; Hypoxia; Oxygen consumption; Rust; Unconsciousness
Abstract
(Druelle A, Daubresse L, Mullot JU, Streit H, Louge P. Hypoxic loss of consciousness in air diving: two cases of mixtures made hypoxic by oxidation of the scuba diving cylinder. Diving and Hyperbaric Medicine. 2023 December 20;53(4):356−359. doi: 10.28920/dhm53.4.356-359. PMID: 38091597. PMCID: PMC10944661.)
Without an adequate supply of oxygen from the scuba apparatus, humans would not be able to dive. The air normally contained in a scuba tank is dry and free of toxic gases. The presence of liquid in the tank can cause corrosion and change the composition of the gas mixture. Various chemical reactions consume oxygen, making the mixture hypoxic. We report two cases of internal corrosion of a scuba cylinder rendering the respired gas profoundly hypoxic and causing immediate hypoxic loss of consciousness in divers.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Case report
Diving Hyperb Med. 2023 December 20;53(4):360. doi: 10.2980/dhm53.4.360. PMID: 38091598. PMCID: PMC10944660.
University of Auckland Postgraduate Diploma in Diving and Hyperbaric Medicine
Michael Davis
Corresponding address: PO Box 35, Tai Tapu 7645, New Zealand
Keywords
Diving medicine; Hyperbaric medicine; Education; Qualifications
Copyright: This article is the copyright of the author who grants Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Letter to the Editor
- Super User
- Category: Information
- 2386
Click to download each article. This will download a PDF that is password protected from any changes, these individual article PDFs are not for public distribution and for society members personal use.
Copyright: These articles are the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
- Super User
- Category: Information
- 12344
2024 March;54(1)
Diving Hyperb Med. 2024 31 March;54(1):2−8. doi: 10.28920/dhm54.1.2-8. PMID: 38507904. PMCID: PMC11227965.
Efficacy of searching in biomedical databases beyond MEDLINE in identifying randomised controlled trials on hyperbaric oxygen treatment
Hira Khan1, Mohammad Sindeed Islam2, Manvinder Kaur3, Joseph K Burns1,3, Cole Etherington1,3, Pierre-Marc Dion2, Sarah Alsayadi4, Sylvain Boet1,3,5,6
1 Clinical Epidemiology Program, Ottawa Hospital Research Institute, Ottawa, ON, Canada
2 Faculty of Medicine, University of Ottawa, Ottawa, ON, Canada
3 Department of Anesthesiology and Pain Medicine, The Ottawa Hospital, Ottawa, ON, Canada
4 Faculty of Science, University of Ottawa, Ottawa, ON, Canada
5 Department of Innovation in Medical Education, University of Ottawa, Ottawa, ON, Canada
6 Institut du Savoir Montfort, Ottawa, ON, Canada
Corresponding author: Dr Sylvain Boet, 1053 Carling Avenue, Ottawa, ON K1Y 4E9, ON, Canada
Keywords
Biomedical databases; Research methods; Systematic review
Abstract
(Khan K, Islam MS, Kaur M, Burns JK, Etherington C, Dion P-M, Alsayadi S, Boet S. Efficacy of searching in biomedical databases beyond MEDLINE in identifying randomised controlled trials on hyperbaric oxygen treatment. Diving and Hyperbaric Medicine. 2024 31 March;54(1):2−8. doi: 10.28920/dhm54.1.2-8. PMID: 38507904. PMCID: PMC11227965.)
Introduction: Literature searches are routinely used by researchers for conducting systematic reviews as well as by healthcare providers, and sometimes patients, to quickly guide their clinical decisions. Using more than one database is generally recommended but may not always be necessary for some fields. This study aimed to determine the added value of searching additional databases beyond MEDLINE when conducting a literature search of hyperbaric oxygen treatment (HBOT) randomised controlled trials (RCTs).
Methods: This study consisted of two phases: a scoping review of all RCTs in the field of HBOT, followed by a a statistical analysis of sensitivity, precision, ‘number needed to read’ (NNR) and ‘number unique’ included by individual biomedical databases. MEDLINE, Embase, Cochrane Central Register of Control Trials (CENTRAL), and Cumulated Index to Nursing and Allied Health Literature (CINAHL) were searched without date or language restrictions up to December 31, 2022. Screening and data extraction were conducted in duplicate by pairs of independent reviewers. RCTs were included if they involved human subjects and HBOT was offered either on its own or in combination with other treatments.
Results: Out of 5,840 different citations identified, 367 were included for analysis. CENTRAL was the most sensitive (87.2%) and had the most unique references (7.1%). MEDLINE had the highest precision (23.8%) and optimal NNR (four). Among included references, 14.2% were unique to a single database.
Conclusions: Systematic reviews of RCTs in HBOT should always utilise multiple databases, which at minimum include MEDLINE, Embase, CENTRAL and CINAHL.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Diving Hyperb Med. 2024 31 March;54(1):9−15. doi: 10.28920/dhm54.1.9-15. PMID:38507905. PMCID: PMC11227964.
Hyperbaric oxygen treatment for infants: retrospective analysis of 54 patients treated in two tertiary care centres
Kubra Ozgok Kangal1, Bengusu Mirasoglu2
1 Department of Underwater and Hyperbaric Medicine, University of Health Sciences, Gulhane Faculty of Medicine, Gulhane Research and Training Hospital, Ankara, Turkey
2 Department of Underwater and Hyperbaric Medicine, Istanbul University, Istanbul Faculty of Medicine, Istanbul, Turkey
Corresponding author: Associate Professor Kubra Ozgok Kangal, Gen. Dr. Tevfik Saglam Cad. SBÜ-Gülhane Eğitim ve Araştırma Hastanesi, Sualtı Hekimliği ve Hiperbarik Tıp Kliniği, Etlik/Ankara, Turkey
Keywords
Hyperbaric medicine; Neonate; Newborn; Premature
Abstract
(Ozgok Kangal K, Mirasoglu B. Hyperbaric oxygen treatment for infants: retrospective analysis of 54 patients treated in two tertiary care centres. Diving and Hyperbaric Medicine. 2024 31 March;54(1):9−15. doi: 10.28920/dhm54.1.9-15. PMID:38507905. PMCID: PMC11227964.)
Introduction: We aimed to analyse the outcomes of hyperbaric oxygen treatment (HBOT) and describe difficulties encountered in infants, a rare patient population in this therapeutic intervention, with limited scientific reports.
Methods: This was a retrospective analysis of patients 12 months old or younger who underwent HBOT in two different institutions. Demographic data, clinical presentation, HBOT indication, chamber type, oxygen delivery method, total number of treatments, outcome and complications were extracted from clinical records.
Results: There were 54 infants in our study. The patients’ median age was 3.5 (range 0–12) months. The major HBOT indication was acute carbon monoxide intoxication (n = 32). A total of 275 HBOT treatments were administered, mostly performed in multiplace chambers (n = 196, 71%). Only one patient (2%) required mechanical ventilation. Acute signs were fully resolved in the most patients (n = 40, 74%). No complications related to HBOT were reported.
Conclusions: This study suggests that HBOT may be a safe and effective treatment for infants. Paediatricians should consider HBOT when indicated in infants even for the preterm age group.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Diving Hyperb Med. 2024 31 March;54(1):16−22. doi: 10.28920/dhm54.1.16-22. PMID: 38507906. PMCID: PMC11227960.
Effect of hyperbaric oxygen treatment on ischaemia-reperfusion injury in rats detorsioned after experimental ovarian torsion
Eralp Bulutlar1, Ali Yilmaz2, Gizem Berfin Uluutku Bulutlar3, Yavuz Aslan4, Hale Nur Bozdağ5, Zafer Küçükodaci6
1 Zeynep Kamil Gynecology and Obstetrics Training and Research Hospital, İstanbul, Turkey
2 Kartal Lütfü Kırdar Training and Research Hospital İstanbul, Turkey
3 Haydarpaşa Numune Training and Research Hospital, İstanbul, Turkey
4 Sultan Abdulhamid Han Research and Training Hospital
5 VM Medical Park Maltepe Hastanesi, İstanbul , Turkey
6 Anadolu Sağlık Merkezi, Gebze, Kocaeli, Turkey
Corresponding author: Dr Eralp Bulutlar, Başakşehir Çam and Sakura City Hospital, Başakşehir Olimpiyat Bulvarı Yolu, 34480 Başakşehir, İstanbul, Turkey
ORCiD: 0000-0002-2246-4899
Keywords
Animal model; Antioxidants; Experimental; Hyperbaric research; Inflammation
Abstract
(Bulutlar E, Yilmaz A, Uluutku Bulutlar GB, Aslan Y, Bozdağ HN, Küçükodaci Z. Effect of hyperbaric oxygen treatment on ischaemia-reperfusion injury in rats detorsioned after experimental ovarian torsion. Diving and Hyperbaric Medicine. 2024 31 March;54(1):16−22. doi: 10.28920/dhm54.1.16-22. PMID: 38507906. PMCID: PMC11227960.)
Introduction: This study aimed to investigate whether hyperbaric oxygen treatment (HBOT) could ameliorate ischaemia-reperfusion injury in a rat model of ovarian torsion-detorsion.
Methods: Twenty-seven rats were divided among four groups: surgical sham rats (S) (n = 6) underwent identical anaesthesia and surgical incisions to other groups (n = 7 per group) but with no ovary intervention; torsion rats (T) underwent laparotomy, ovarian torsion, relaparotomy and sacrifice after three hours; torsion and detorsion rats (T/DT) underwent laparotomy, ovarian torsion (three hours), relaparotomy and detorsion, and sacrifice after one week; torsion, detorsion, hyperbaric oxygen rats (T/DT/HBOT) underwent laparotomy, ovarian torsion, relaparotomy and detorsion, and sacrifice after one week during which HBOT was provided 21 times (100% oxygen at 600 kPa for 50 min). In all groups blood collection for markers of oxidative stress or related responses, and ovary collection for histology were performed after sacrifice.
Results: When the T/DT, and T/DT/HBOT groups were compared, 8-hydroxy-2′-deoxyguanosine (a marker of oxidative damage to DNA) and malondialdehyde (a product of lipid peroxidation) levels were lower in the T/DT/HBOT group. Anti-Mullerian hormone levels were higher in the T/DT/HBOT group compared to the T/DT group. In addition, oedema, vascular occlusion, neutrophilic infiltration and follicular cell damage were less in the T/DT/HBOT group
than in the T/DT group.
Conclusions: When biochemical and histopathological findings were evaluated together, HBOT appeared reduce ovarian ischaemia / reperfusion injury in this rat model of ovarian torsion-detorsion.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Diving Hyperb Med. 2024 31 March;54(1):23−38. doi: 10.28920/dhm54.1.23-38. PMID: 38507907. PMCID: PMC11065503.
Review of saturation decompression procedures used in commercial diving
Jean-Pierre Imbert1, Lyubisa Matity2, Jean-Yves Massimelli3, Philip Bryson4
1 Divetech, 1543 chemin des vignasses, 06410 Biot, France
2 Hyperbaric and Tissue Viability Unit, Gozo General Hospital, Malta
3 CHU de Nice, Hôpital Pasteur, 30 avenue de la voie romaine, 06001 Nice, France
4 International SOS, Forest Grove House, Foresterhill Road, Aberdeen, AB25 2ZP, UK
Corresponding author: Jean Pierre Imbert, Divetech, 1543 ch des vignasses 0641Biot, France
Keywords
Decompression tables; Occupational diving; Saturation diving
Abstract
(Imbert J-P, Matity L, Massimelli J-Y, Bryson P. Review of saturation decompression procedures used in commercial diving. Diving and Hyperbaric Medicine. 2024 31 March;54(1):23−38. doi: 10.28920/dhm54.1.23-38. PMID: 38507907. PMCID: PMC11065503.)
Introduction: This is a review of commercial heliox saturation decompression procedures. The scope does not include compression, storage depth or bell excursion dive procedures. The objectives are to: identify the sources of the procedures; trace their evolution; describe the current practice; and detect relevant trends.
Methods: Eleven international commercial diving companies provided their diving manuals for review under a confidentiality agreement.
Results: Modern commercial diving saturation procedures are derived from a small number of original procedures (United States Navy, Comex, and NORSOK). In the absence of relevant scientific studies since the late 80’s, the companies have empirically adapted these procedures according to their needs and experience. Such adaptation has caused differences in decompression rates shallower than 60 msw, decompression rest stops and the decision to decompress linearly or stepwise. Nevertheless, the decompression procedures present a remarkable homogeneity in chamber PO2 and daily decompression rates when deeper than 60 msw. The companies have also developed common rules of good practice; no final decompression should start with an initial ascending excursion; a minimum hold is required before starting a final decompression after an excursion dive. Recommendation is made for the divers to exercise during decompression.
Conclusions: We observed a trend towards harmonisation within the companies that enforce international procedures, and, between companies through cooperation inside the committees of the industry associations.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Full article available here.
Diving Hyperb Med. 2024 31 March;54(1):39−46. doi: 10.28920/dhm54.1.39-46. PMID: 38507908. PMCID: PMC11227959.
Chain of events analysis in diving accidents treated by the Royal Netherlands Navy 1966–2023
Benjamin L Turner1, Pieter-Jan AM van Ooij1,2, Thijs T Wingelaar1,3, Rob A van Hulst3, Edwin L Endert1, Paul Clarijs1, Rigo Hoencamp4,5,6
1 Royal Netherlands Navy Diving and Submarine Medical Centre, Den Helder, The Netherlands
2 Department of Respiratory Medicine, Amsterdam UMC, Location AMC, University of Amsterdam, Amsterdam, The Netherlands
3 Department of Anesthesiology, Amsterdam UMC, Location AMC, University of Amsterdam, Amsterdam, The Netherlands
4 Department of Surgery, Alrijne Hospital, Leiderdorp, the Netherlands
5 Trauma Research Unit, Department of Trauma Surgery, Erasmus MC, University Medical Center Rotterdam, Rotterdam, the Netherlands
6 Defence Healthcare Organization, Ministry of Defence, Utrecht, the Netherlands
Corresponding author: Mr Benjamin L Turner, Royal Netherlands Navy Diving and Submarine Medical Centre, Den Helder, The Netherlands
ORCiD: 0009-0004-6606-9788
Keywords
Arterial gas embolism; Decompression sickness; Incidents; Risk factors; Safety; Underwater hazards
Abstract
(Turner BL, van Ooij P-JAM, Wingelaar TT, van Hulst RA, Endert EL, Clarijs P, Hoencamp R. Chain of events analysis in diving accidents treated by the Royal Netherlands Navy 1966-2023. Diving and Hyperbaric Medicine. 2024 31 March;54(1):39−46. doi: 10.28920/dhm54.1.39-46. PMID: 38507908. PMCID: PMC11227959.)
Introduction: Diving injuries are influenced by a multitude of factors. Literature analysing the full chain of events in diving accidents influencing the occurrence of diving injuries is limited. A previously published ‘chain of events analysis’ (CEA) framework consists of five steps that may sequentially lead to a diving fatality. This study applied four of these steps to predominately non-lethal diving injuries and aims to determine the causes of diving injuries sustained by divers treated by the Diving Medical Centre of the Royal Netherlands Navy.
Methods: This retrospective cohort study was performed on diving injuries treated by the Diving Medical Centre between 1966 and 2023. Baseline characteristics and information pertinent to all four steps of the reduced CEA model were extracted and recorded in a database.
Results: A total of 288 cases met the inclusion criteria. In 111 cases, all four steps of the CEA model could be applied. Predisposing factors were identified in 261 (90%) cases, triggers in 142 (49%), disabling agents in 195 (68%), and 228 (79%) contained a (possible-) disabling condition. The sustained diving injury led to a fatality in seven cases (2%). The most frequent predisposing factor was health conditions (58%). Exertion (19%), primary diver errors (18%), and faulty equipment (17%) were the most frequently identified triggers. The ascent was the most frequent disabling agent (52%).
Conclusions: The CEA framework was found to be a valuable tool in this analysis. Health factors present before diving were identified as the most frequent predisposing factors. Arterial gas emboli were the most lethal injury mechanism.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Original article
Diving Hyperb Med. 2024 31 March;54(1):47−56. doi: 10.28920/dhm54.1.47-56. PMID: 38507909.
Reported outcome measures in necrotising soft tissue infections: a systematic review
Jonathan Wackett1, Bridget Devaney2,3,4, Raymond Chau5, Joshua Ho5, Nicholas King5, Jasleen Grewal1, Joshua Armstrong6, Biswadev Mitra2,4
1 Department of Medicine, Alfred Health, Melbourne, Australia
2 Emergency and Trauma Centre, Alfred Health, Melbourne, Australia
3 Department of Intensive Care and Hyperbaric Medicine, Alfred Health, Melbourne, Australia
4 Department of Epidemiology and Preventative Medicine, Monash University, Melbourne, Australia
5 Monash Health, Melbourne, Australia
6 Barwon Health, Geelong, Australia
Corresponding author: Dr Bridget Devaney, Head of Hyperbaric Medicine, Alfred Health, 55 Commercial Road, Melbourne, VIC 3004, Australia
ORCiD: 0000-0001-6521-418X
Keywords
Fournier’s gangrene; Gas gangrene; Hyperbaric oxygen treatment; Intensive care medicine; Systematic review
Abstract
(Wackett J, Devaney B, Chau R, Ho J, King N, Grewal J, Armstrong J, Mitra B. Reported outcome measures in necrotising soft tissue infections: a systematic review. Diving and Hyperbaric Medicine. 2024 31 March;54(1):47−56. doi: 10.28920/dhm54.1.47-56. PMID: 38507909. PMCID: PMC11371474.)
Introduction: There are inconsistencies in outcome reporting for patients with necrotising soft tissue infections (NSTI). The aim of this study was to evaluate reported outcome measures in NSTI literature that could inform a core outcome set (COS) such as could be used in a study of hyperbaric oxygen in this indication.
Methods: A systematic review of all NSTI literature identified from Cochrane, Ovid MEDLINE and Scopus databases as well as grey literature sources OpenGrey and the New York Academy of Medicine databases which met inclusion criteria and were published between 2010 and 2020 was performed. Studies were included if they reported on > 5 cases and presented clinical endpoints, patient related outcomes, or resource utilisation in NSTI patients. Studies did not have to include intervention. Two independent researchers then extracted reported outcome measures. Similar outcomes were grouped and classified into domains to produce a structured inventory. An attempt was made to identify trends in outcome measures over time and by study design.
Results: Three hundred and seventy-five studies were identified and included a total of 311 outcome measures. Forty eight percent (150/311) of outcome measures were reported by two or more studies. The four most frequently reported outcome measures were mortality without time specified, length of hospital stay, amputation performed, and number of debridements, reported in 298 (79.5%), 260 (69.3%), 156 (41.6%) and 151 (40.3%) studies respectively. Mortality outcomes were reported in 23 different ways. Randomised controlled trials (RCTs) were more likely to report 28-day mortality or 90-day mortality. The second most frequent amputation related outcome was level of amputation, reported in 7.5% (28/375) of studies. The most commonly reported patient-centred outcome was the SF-36 which was reported in 1.6% (6/375) of all studies and in 2/10 RCTs.
Conclusions: There was wide variance in outcome measures in NSTI studies, further highlighting the need for a COS.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Review article
Diving Hyperb Med. 2024 31 March;54(1):57−60. doi: 10.28920/dhm54.1.57-60. PMID: 38507910. PMCID: PMC11227961.
Equipoise: an important ethical consideration when contemplating participation in a randomised controlled trial of hyperbaric oxygen treatment in necrotising soft tissue infections
Bridget Devaney1,2,3
1 Emergency and Trauma Centre, Alfred Health, Melbourne, Australia
2 Department of Intensive Care and Hyperbaric Medicine, Alfred Health, Melbourne, Australia
3 Department of Epidemiology and Preventative Medicine, Monash University, Melbourne, Australia
Corresponding author: Dr Bridget Devaney, Head of Hyperbaric Medicine, Alfred Health, 55 Commercial Road, Melbourne, VIC 3004, Australia
ORCiD: 0000-0001-6521-418X
Keywords
Clinical trials; Ethics; Hyperbaric research
Abstract
(Devaney B. Equipoise: an important ethical consideration when contemplating participation in a randomised controlled trial of hyperbaric oxygen treatment in necrotising soft tissue infections. Diving and Hyperbaric Medicine. 2024 31 March;54(1):57−60. doi: 10.28920/dhm54.1.57-60. PMID: 38507910. PMCID: PMC11227961.)
A proposal for a large, multi-centre, randomised controlled trial investigating the role of hyperbaric oxygen treatment (HBOT) in necrotising soft tissue infections (NSTI) has led to much discussion locally and internationally about whether participation is ethical for a centre where stakeholders already consider HBOT standard practice. This article systematically addresses the concept of clinical equipoise specific to the role of HBOT in NSTI, and presents a series of considerations to be taken into account by key stakeholders at potential participating sites.
Copyright: This article is the copyright of the author who grants Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: World as it is
Diving Hyperb Med. 2024 31 March;54(1):61−64. doi: 10.28920/dhm54.1.61-64. PMID: 38507911. PMCID: PMC11227966.
Secondary deterioration in a patient with cerebral and coronary arterial gas embolism after brief symptom resolution: a case report
Ryota Tsushima1, Kosuke Mori2, Shohei Imaki1
1 Yokohama Municipal Citizen’s Hospital 1-1, Mitsuzawanishi-chou, Kanagawa-ku, Yokohama-city, Kanagawa-ken 221-0855, Japan
2 Yokohama Minami Kyosai Hospital 1-21-1, Mutsurahigashi, Kanazawa-ku, Yokohama- city, Kanagawa-ken 236-0037, Japan
Corresponding author: Dr Ryota Tsushima, Yokohama Municipal Citizen’s Hospital 1-1, Mitsuzawanishi-chou, Kanagawa-ku, Yokohama-city, Kanagawa-ken 221-0855, Japan
Keywords
Air embolism; Case reports; Hyperbaric oxygen treatment
Abstract
(Tsushima R, Mori K, Imaki S. Secondary deterioration in a patient with cerebral and coronary arterial gas embolism after brief symptom resolution: a case report. Diving and Hyperbaric Medicine. 2024 31 March;54(1):61−64. doi: 10.28920/dhm54.1.61-64. PMID: 38507911. PMCID: PMC11227966.)
Introduction: Hyperbaric oxygen treatment (HBOT) is recommended for arterial gas embolism (AGE) with severe symptoms. However, once symptoms subside, there may be a dilemma to treat or not.
Case presentation: A 71-year-old man was noted to have a mass shadow in his left lung, and a transbronchial biopsy was performed with sedation. Flumazenil was intravenously administered at the end of the procedure. However, the patient remained comatose and developed bradycardia, hypotension, and ST-segment elevation in lead II. Although the ST changes spontaneously resolved, the patient had prolonged disorientation. Whole- body computed tomography revealed several black rounded lucencies in the left ventricle and brain, confirming AGE. The patient received oxygen and remained supine. His neurological symptoms gradually improved but worsened again, necessitating HBOT. HBOT was performed seven times, after which neurological symptoms resolved almost completely.
Conclusions: AGE can secondarily deteriorate after symptoms have subsided. We recommend that HBOT be performed promptly once severe symptoms appear, even if they resolve spontaneously.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Case report
Diving Hyperb Med. 2024 31 March;54(1):65−68. doi: 10.28920/dhm54.1.65-68. PMID: 38507912. PMCID: PMC11227963.
Hyperbaric oxygen for the treatment of carbon monoxide-induced delayed neurological sequelae: a case report and review of the literature
Zebedee KR Wong1, Colin KA Teo1, James WM Kwek1, Soo Joang Kim2, Hooi Geok See3
1 Navy Medical Service, Republic of Singapore Navy, Singapore
2 Hyperbaric and Diving Medicine Centre, Singapore General Hospital, Singapore
3 Division of Anaesthesiology and Perioperative Medicine, Singapore General Hospital, Singapore
Corresponding author: Dr Zebedee KR Wong, Navy Medical Service, Republic of Singapore Navy, Singapore
ORCiD: 0009-0000-0081-3915
Keywords
Hyperbaric medicine; Morbidity; Pain; Neurology; Psychology; Radiological imaging; Toxicity
Abstract
(Wong ZKR, Teo CKA, Kwek JWM, Kim SJ, See HG. Hyperbaric oxygen for the treatment of carbon monoxide-induced delayed neurological sequelae: a case report and review of the literature. Diving and Hyperbaric Medicine. 2024 31 March;54(1):65−68. doi: 10.28920/dhm54.1.65-68. PMID: 38507912. PMCID: PMC11227963.)
Introduction: Hyperbaric oxygen treatment (HBOT) remains a recognised treatment for acute carbon monoxide (CO) poisoning, but the utility of HBOT in treating CO-induced delayed neurological sequelae (DNS) is not yet established.
Case description: A 26-year old woman presented with reduced consciousness secondary to CO exposure from burning charcoal. She underwent a single session of HBOT with US Navy Treatment Table 5 within six hours of presentation, with full neurological recovery. Eight weeks later, she represented with progressive, debilitating neurological symptoms mimicking Parkinsonism. Magnetic resonance imaging of her brain demonstrated changes consistent with hypoxic ischaemic encephalopathy. The patient underwent 20 sessions of HBOT at 203 kPa (2 atmospheres absolute) for 115 minutes, and received intravenous methylprednisolone 1 g per day for three days. The patient’s neurological symptoms completely resolved, and she returned to full-time professional work with no further recurrence.
Discussion: Delayed neurological sequelae is a well-described complication of CO poisoning. In this case, the patient’s debilitating neurocognitive symptoms resolved following HBOT. Existing literature on treatment of CO-induced DNS with HBOT consists mainly of small-scale studies and case reports, many of which similarly suggest that HBOT is effective in treating this complication. However, a large, randomised trial is required to adequately determine the effectiveness of HBOT in the treatment of CO-induced DNS, and an optimal treatment protocol.
Copyright: This article is the copyright of Case report
Diving Hyperb Med. 2024 31 March;54(1):69−72. doi: 10.28920/dhm54.1.69-72. PMID: 38507913. PMCID: PMC11065502.
The first deep rebreather dive using hydrogen: case report
Richard J Harris1, Craig J Challen1, Simon J Mitchell1,2,3,4
1 Technical diver, Wetmules Dive Team
2 Department of Anaesthesiology, School of Medicine, University of Auckland, Auckland, New Zealand
3 Department of Anaesthesia, Auckland City Hospital, Auckland, New Zealand
4 Slark Hyperbaric Unit, North Shore Hospital, Auckland, New Zealand
Corresponding author: Professor Simon Mitchell, Department of Anaesthesiology, School of Medicine, University of Auckland, Private Bag 92019, Auckland 1142, New Zealand
ORCiD: 0000-0002-5149-6371
Keywords
Helihydrox; High pressure neurological syndrome; HPNS; Hydreliox; Hydrox; Technical diving; Trimix
Abstract
(Harris RJ, Challen CJ, Mitchell SJ. The first deep rebreather dive using hydrogen: case report. Diving and Hyperbaric Medicine. 2024 31 March;54(1):69−72. doi: 10.28920/dhm54.1.69-72. PMID: 38507913. PMCID: PMC11065502.)
Bounce diving with rapid descents to very deep depths may provoke the high-pressure neurological syndrome (HPNS). The strategy of including small fractions of nitrogen in the respired gas to produce an anti-HPNS narcotic effect increases the gas density which may exceed recommended guidelines. In 2020 the ‘Wetmules’ dive team explored the Pearse Resurgence cave (New Zealand) to 245 m breathing trimix (approximately 4% oxygen, 91% helium and 5% nitrogen). Despite the presence of nitrogen, one diver experienced HPNS tremors beyond 200 m. The use of hydrogen (a light yet slightly narcotic gas) has been suggested as a solution to this problem but there are concerns, including the potential for ignition and explosion of hydrogen-containing gases, and accelerated heat loss. In February 2023 a single dive to 230 m was conducted in the Pearse Resurgence to experience hydrogen as a breathing gas in a deep bounce dive. Using an electronic closed-circuit rebreather, helihydrox (approximately 3% oxygen, 59% helium and 38% hydrogen) was breathed between 200 and 230 m. This was associated with amelioration of HPNS symptoms in the vulnerable diver and no obvious adverse effects. The use of hydrogen is a potential means of progressing deeper with effective HPNS amelioration while maintaining respired gas density within advised guidelines.
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Case report
Full article available here.
Diving Hyperb Med. 2024 March 31;54(1):73−74. doi: 10.28920/dhm54.1.73-74. PMID: 38507914.
Time to shock people
Gerard Laden1, Bruce Mathew1, Ananthakrishnan Ananthasayanam1,2
1 Clinical Hyperbaric Facility, Hull and East Riding Hospital, Anlaby, UK
2 Department of Surgery, Hull University Teaching Hospitals, NHS Trust, Hull, UK
Corresponding author: Mr Gerard Laden, Clinical Hyperbaric Facility, Hull and East Riding Hospital, Anlaby, UK
ORCiD: 0009-0008-0820-8291
Keywords
Cardiac; CPR, Defibrillation; First aid; Resuscitation
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Letter to the Editor
Diving Hyperb Med. 2024 March 31;54(1):74−75. doi: 10.28920/dhm54.1.74-75. PMID: 38507915. PMCID: PMC11227962.
Response to Laden et al.
Andrew Tabner1,2, Graham Johnson1,2, Philip Bryson3 on behalf of the authorship team
1 Emergency Department, Royal Derby Hospital, Uttoxeter Road, Derby, UK, DE22 3NE
2 University of Nottingham Medical School, Queen’s Medical Centre, Nottingham, UK, NG7 2UH
3 TAC Healthcare, Wellheads Crescent, Aberdeen, Scotland AB21 7GA
Corresponding author: Dr Andrew Tabner, Emergency Department, Royal Derby Hospital, Uttoxeter Road, Derby, UK, DE22 3NE
Keywords
Resuscitation; Defibrillation; Mechanical CPR; Cardiovascular; Letters (to the Editor)
Copyright: This article is the copyright of the authors who grant Diving and Hyperbaric Medicine a non-exclusive licence to publish the article in electronic and other forms.
Publication Type: Letter to the Editor